After police shot and killed a Charlotte man who was deaf last year, some North Carolina lawmakers want to take a closer look at law enforcement mental health and disability training.
House Bill 591 would direct the state Departments of Justice and Public Safety to study different types of training available for officers to improve their traffic stop interactions with individuals with disabilities. The bill, sponsored by Rep. Charles Graham (D-Lumberton), passed through the House Health committee last week.
Rep. Charles Graham (R-Lumberton)
Graham worked with students with special needs in Robeson County for 31 years and said many of his students went on to receive a driver’s license. He cited oppositional defiance disorder, traumatic brain injury and post-traumatic stress disorder as just a few of the issues that affect a person’s ability to interact with a police officer.
“Just because you become a certain age to have a driver’s license doesn’t mean that diagnosis disappears,” he said. “A person always carries that diagnosis.”
“Not all drivers have normal functional and cognitive abilities,” Graham said. “Although they have a driver’s license — and they are entitled to have the driver’s license — they don’t have what we consider to be normal behavioral interactions.”
That phenomenon was in evidence during another incident in Charlotte last year, where a man acting erratically was shot and killed by police; it was later discovered that he had a traumatic brain injury.
Raleigh CIT officer Wendy Clark and counselor Benny Langdon demonstrate how to handle an intoxicated, combative man during the Wake County CIT training in 2013. Photo credit: Rose Hoban
During last week’s committee meeting, Rep. Cynthia Ball (D-Raleigh) spoke in support of Graham’s bill, adding that she sponsored legislation that would create a designation on driver’s licenses to identify deaf and hearing impaired drivers. House Bill 84 has already passed the House and is moving through the Senate.
Rep. Jay Adams (R-Hickory) asked if lawmakers should be studying “at what point a person is not eligible for a driver’s license […] Are there people out there who are licensed to drive that are virtually going to be impossible to deal with?”
Graham said that is not within the scope of this study bill. Its goal is to determine whether law enforcement needs a certain level of mental health and disability training, and if so, what should that be.
“I don’t think we can put a label on a person and say, ‘because you have PTSD, you’re not eligible for a driver’s license,'” Graham said. “I don’t want to imply that’s what this study is about.”
“We have people that go into law enforcement with a high school diploma,” he added. “They have no knowledge of what PTSD is. The have no knowledge of what some of these diagnosis might carry.”
All law enforcement officers have a mental health awareness course during basic training. About 45 percent go through additional Crisis Intervention Training (CIT), a more robust course available across the state for any interested officers. It teaches them skills such as how to de-escalate a situation.
By the end of last year, 9,536 North Carolina law enforcement officers completed the CIT program out of about 21,000 full-time officers, according to the N.C. Department of Health and Human Services.
Rep. Beverly Boswell (R-Kill Devil Hills)
The North Carolina chapter of the National Alliance on Mental Illness helps revise the curriculum for the CIT program every few years. NAMI NC Executive Director Jack Register said his organization always supports study legislation like House Bill 591, especially because CIT is the only real training in the state. So exploring options is welcome.
Rep. Beverly Boswell (R- Kill Devil Hills) was the only lawmaker in the committee to vote against the bill on Tuesday.
“When a police officer pulls you over, he asks that you follow simple commands,” Boswell said. “So is that the issue? Or are we going to make the police officers a medical provider? Because that’s a very thin line.
“All drivers have to obey the same rules and regulations” she added. “So if they are unable to follow the commands of a police officer how can they have a valid driver’s license?”
Matthew Herr, policy analyst with Disability Rights, spoke in support of the bill. He said when it comes to someone with autism, for example, “they may be able to follow commands but it may take them longer, or they may have some informational processing limitations that slows down their reaction.”
He pointed out that there is already a medical review process in place at the North Carolina Division of Motor Vehicles.
But Herr noted there is not a consensus among disability advocates about how law enforcement should approach these individuals, which is why he thinks a study is so needed.
“When we say people with disabilities, it’s deceptively complex term,” he said. “The best practices for dealing with a person with autism may be different than the best practices for dealing with a person with severe anxiety.”
State environmental regulators are investigating how to stop the release of air emissions carrying compounds related to GenX from the Chemours manufacturing site in Bladen County that chemical giant DuPont ran for decades.
That’s because those emissions may be contributing to contamination detected in recent months in private drinking wells close to the facility, as well as in public drinking water systems downstream that draw from the Cape Fear River.
Department of Environmental Quality air specialists are researching techniques that could capture emissions of a long list of unregulated perfluorinated compounds, known as PFAS, from multiple smokestacks on the 2,200-acre site, said agency air quality division director Mike Abraczinskas.
Data that DEQ requested from Chemours suggests practically no GenX was released into the atmosphere from 2012 to 2016. But other unregulated compounds have been emitted, including one discharged at levels reaching 75,000 pounds in one year.
DEQ and the state Department of Health and Human Services will host a third community information session on its well testing program near Chemours at 6 pm Thursday, Dec. 14, at Gray’s Creek High School auditorium in Hope Mills.
Figuring out whether any of those compounds pose risks to people could take a very long time. So in the shorter term, DEQ wants to guide Chemours on what pollution controls the company can use to stop the emissions, Abraczinskas said during an interview with NC Health News last week.
“We’re asking: how can we eliminate or destroy all of these before they are emitted,” he said.
Airborne concerns
It could be that air emissions that regulators don’t yet understand might be the culprit behind why Genx has been detected in private wells farther than expected from the Fayetteville Works manufacturing site.
For one thing, the chemical was detected in levels high above North Carolina’s established health goal of 140 parts per trillion in wells on land across the expanse of the Cape Fear River. Normally a river of that size would be a barrier to polluted groundwater moving from one place to another.
Meteorological data collected from 1998 to 2017 at Fayetteville Regional Airport and analyzed by DEQ shows wind patterns that cross the Chemours site. Those breezes would likely have moved any emissions to the northeast and southwest of the industrial property, and over locations where well tests are now turning up positive for GenX.
Chemours emission estimates created by DEQ with a widely accepted computer model suggests only very small amounts of GenX and very closely related compounds have been emitted from the facility.
The state Department of Environmental Quality wants to confirm this Chemours estimate of GenX and similar compound emissions with stack testing the company will perform with equipment and procedures DEQ endorses. Source: DEQ
But it’s also known that one of these chemicals, known as C3 dimer acid fluoride, can convert to GenX after contact with water. What’s not known is whether any of that compound released from the Chemours facility was transformed this way, Abraczinskas said.
“If you emit it as a gas, how quickly will it convert to GenX?” Abraczinskas asked. “Does it happen in the presence of water vapor, with rain, or does it have to deposit in a puddle? We’re asking universities, the EPA and the company. We don’t have answers yet.”
To confirm the Chemours estimates, the state is having the company sample for any GenX that gets past the smokestack scrubbing equipment during normal operations.
Meteorological data from Fayetteville Regional Airport has helped state regulators predict where air emissions from Chemours are most likely to be found. Source: DEQ
Last month DEQ Secretary Michael Regan moved to revoke a significant portion of Chemours’ permit to discharge wastewater into the Cape Fear after the company failed to report a spill that elevated its GenX discharges into the Cape Fear River. DEQ asked the State Bureau of Investigation to investigate if Chemours broke any criminal law by not disclosing the release.
New players
Also of interest is a long list of related compounds the facility released into the air between 2012 and 2016, data that the company recently collated for DEQ. One of particular note is hexafluoropropylene oxide (HFPO), whose release reached 72,500 pounds in 2015 and 42,119 pounds in 2016.
DEQ leaders Michael Scott with the waste management division, Linda Culpepper with water resources and Mike Abraczinskas with air quality speak with state Rep. Pricey Harrison, (D-Greensboro), in blue, after a meeting of the House Special Select Committee on North Carolina River Quality last week. Source: DEQ
“The question is what does that stuff do?” Abraczinskas said of the HFPO emissions. “We know it’s an essential building block to a lot of things they make. Does it have the potential to form GenX in any way? We’re trying to find out.”
A DuPont brochure says HFPO can be used to produce perfluorinated vinyl ethers which are used in the production of commercial fluoropolymers, which are used in thousands of products, including non-stick coatings such as Teflon.
Sponsored
Last summer, a Chemours representative told state and locals officials that GenX detected in the Cape Fear was a byproduct of one of these vinyl ether processes. But he noted that particular process was exempted from an EPA order that Chemours not release GenX into the environment due to potential health concerns.
Eager for a fix
State Rep. Ted Davis (R-Wilmington) last week said he does not agree with some people who are calling for Chemours to be shut down. At the same time, he said steps must be taken to ensure that people are not exposed to dangerous industrial chemicals originating there.
Rep. Ted Davis, Jr. (R-Wilmington)
“You’ve got to weigh the safety of the people with the benefits of that industry being here,” said Davis who co-chairs a House committee on Clean Rivers, created after news of GenX contamination broke. “To me, it makes sense to let the company operate but take that stuff elsewhere.”
Neighbors to the Chemours compound are carefully watching everything state officials are doing to eliminate and, eventually, clean up any pollution close to their homes.
Many are alarmed by the results of well tests that DEQ Assistant Secretary Sheila Holman reported last week during a meeting of the House Select Committee on River Quality, which Davis co-chairs.
In a first round of testing starting in September, 51 out of 141 wells had concentrations of GenX above the state’s provisional health goal; 35 had no GenX detected. A second round begun in October expanded sampling to 450 properties within one mile of Chemours’ property line. As of last week, 34 out of 107 wells sampled had concentrations of GenX above the state’s health goal; only 25 showed no GenX.
Chemours, state officials and Bladen and Cumberland County officials have met to discuss how to best get new water supplies into homes whose wells have GenX exceeding the state health goal.
Mike Watters, a founder of Grays Creek Residents United Against GenX in our Wells and Rivers, says Chemours should pay to connect residents to municipal water supplies and compensate them for the equivalent of any property value they’ve lost.
In addition to exposure via water, Watters wondered what air emissions may have done to soils, home vegetable gardens and crops raised to feed livestock. He was disheartened by news Monday that GenX has been detected in food: in honey harvested from a beehive in Robeson County.
Long-term health monitoring of people who live near the plant is going to be vital, he argued.
Members of a committee examining access to care for people in rural North Carolina hit the road last week, bringing lobbyists, lawmakers and legislative staff to Columbus County, two hours southeast of Raleigh, for a hearing.
“Whiteville is a very unique place in that it is a very rural community, still has a very traditional rural-based economy, but it is a community that still is somewhat vibrant,” said committee co-chair Rep. David Lewis (R-Dunn). “So we thought this would let us see the challenges that are faced by even a more successful or more wealthy community. Certainly, if this hospital faces them then one in a poorer community will have more challenges.”
Committee members heard formal presentations from the head of hospitals in Columbus, Robeson and Scotland counties, all facilities serving primarily rural populations. The three counties consistently rank at the very bottom of annual county health rankings, and each has some of the highest rates of poverty in the state.
The three hospital CEOs talked through their telehealth initiatives, the challenges of recruiting and keeping health care providers, and emergency departments jammed with behavioral health patients.
The presentations were followed by a relatively freewheeling lunchtime discussion with the hospital leaders, something usually not allowed for in an ordinary hearing. The CEOs discussed what they need to survive in an increasingly consolidated and competitive health care marketplace marked by non-paying and uninsured patients, decreasing reimbursements from commercial insurance plans, and uncertainty facing governmental payers such as Medicaid and Medicare.
“We’re serious about trying to make a difference and improve access to health care,” Lewis told the CEOs.
Call a doctor
Each hospital leaders described their use of telehealth services to fill some of the gaps in care created by personnel shortages.
Columbus Regional Healthcare System emergency department manager Donna Hill (left) listens as Sen. David Curtis (R-Denver) asks questions about the facility’s telehealth services. Photo credit: Rose Hoban
Veneziano, who relocated last year from New York City, said she never had an appreciation of what these types of services could mean to a rural community.
It costs $12,000 per month just for the telepsychiatry service, Veneziano said. Despite paying for the telestroke and telepsychiatry services to be present in their facilities, she said the hospital can’t bill for them, in part because the services use physicians who are in other states to deliver the consultations.
But Scotland Health Care System CEO Greg Wood said the hospitals can come out ahead, despite the cost. Wood told of how one of his former board members was on the receiving end of telestroke services during the previous week.
“This little R2D2 camera wheeled right in!” Wood said his board member told him. The man thought he was having a stroke. Within two minutes in the ER, he had a neurologist on the line to confirm that he did not need a stroke-busting drug.
The physician on the telestroke service was also able to determine the patient didn’t need to go to a larger medical center to see a neurologist, so he was able to have tests and recuperate in a hospital close to home for several days.
“It worked out well for the patient,” Wood said. “We’d never be able to recruit that capacity to a small town.”
Recruitment strategy: Attract residents
Wood and the others said that problems with recruiting medical talent was ongoing, describing difficulties finding doctors, nurses and other professionals for their facilities.
“We currently need 19 primary care physicians and 11 specialty providers,” said Southeastern Regional Medical Center CEO Joann Anderson. “We have had two OB physicians leave our community; a third is in the process of leaving. That leaves me with one full-time OB/GYN and one GYN.”
Each year, 1,500 babies are delivered at her facility.
“If you Google Robeson County, the statistics that come up are negative statistics, in terms of where you might want to live,” she said.
Anderson’s facility has partnered with Campbell University to provide a place for osteopathic physicians from the new medical school to perform post-academic training. But that comes with a big price tag.
“It was a little over $11 million for this year,” Anderson said. “The cost of that was the salaries for each of the residents, faculty costs, the location, the space that we had to provide for them, all the equipment they had to have. For example, we had to buy three ultrasound machines for them to use, each costs thousands of dollars.”
“A lot of things went into that figure.”
Anderson said she’s only starting to see the return on investment, four of the nine primary care residents completing training will stay there.
Columbus Regional Healthcare System emergency department manager Donna Hill (left) shows committee co-chair Rep. David Lewis around their facility. Photo credit: Rose Hoban
“We have four who have signed to stay in Lumberton, a fifth is in negotiations with me today, two … will stay in North Carolina in the western part of the state,” she said. “That’s just the beginning.”
She also said the hospital had more than 600 applicants for six slots for emergency medical residents.
On top of costs for residents, Anderson said her hospital spent about $8 million on contract nurses last year because of a local shortage.
Wood also spent millions on contract nurses and reiterated the need to train nurses at the local community college to keep them. He also pointed to the increasing trend of hospitals having to hire their physicians. To keep their long-time ear, nose and throat specialist, Wood had to pay dearly.
“He’s been pushing us for three years to help him run his practice, he keeps losing money,” Wood said. “He finally showed up and said I have two offers to leave town. He’s the only ENT in town. Do you want to employ me or do you want to see your ENT service lose?”
To employ him, Wood had to fix up his office, replace his computer system, hire more staff and pay him more.
“I had to go to the board and say, ‘We want to employ this ENT physician, something we used to get for free for his services and it’ll cost us a few hundred thousand dollars,’” he said.
His board approved.
Tip of the iceberg
The CEOs also discussed the skyrocketing costs for behavioral health patients that are currently filling emergency department beds, competition in their urgent care business, and high rates of uninsured, Medicare and Medicaid patients, who bring with them poor reimbursement.
Add to these challenges the federal budget has made cuts to programs to provide loan repayment for providers willing to serve in high poverty rural areas.
After tours of the emergency department and the cancer treatment center, Lewis said he was looking to roll out some relief in the upcoming legislative short session, that begins in May. He mused that the relief might take the form of changes to residency training reimbursement and paying for telehealth services.
“We said, if we can make one thing better, if we can make one person just a little bit healthier, then this will have been well spent,” Lewis said.
Looking for new locations where hunger hits the hardest, planners at Loaves & Fishes, a Charlotte-Mecklenburg County emergency food provider, used a sophisticated, layered mapping process born at UNC-Chapel Hill to find the right spots.
“Access to medical services is crucial to being healthy, but research shows that more than 70 percent of a person’s overall health is driven by social and environmental factors outside the health care system,” Dr. Betsey Tilson, state health director and DHHS chief medical officer, said in a statement.
The layered state guide, called a “story map,” lets users track information from 10 county-based public health regions across the state. The data show the chief non-medical factors — residents’ economic status, social and neighborhood conditions, and housing and transportation access — that can have overriding effects on community health.
Lighting up
“We wanted to make sure that the pantries we operate and those we open are in the right location,” said Tina Postel, executive director of Loaves & Fishes in Charlotte. “One of our pantries that we opened was at Hope Covenant House. It’s in an area that we didn’t have a pantry, but it lit up bright green on the map.”
A look at the DHHS map shows that Region 4, Tract 45 of Mecklenburg County, where the community-development corporation Hope Covenant House is located, is home to 3,146 people. Almost three out of four have poor access to grocery stores, making it a natural market for a new food pantry, Loaves & Fishes decided in 2016, based on data from a pilot map.
Screen shot of the social determinants map showing poor food access in a region of northwest Charlotte.
“We’re taking these findings and data to a larger group of stakeholders to design interventions,” said John Wallace, a data analyst with the Institute for Public Health. “It’s not necessarily guiding the intervention.”
Low access to food was defined for the study as living more than a half mile from a large grocery store in an urban setting, or in a rural setting living more than 10 miles from a large grocery or supercenter.
In contrast to Tract 45 north of downtown Charlotte, everyone of the 2,285 people in Mecklenburg’s Region 4, Tract 58.29, had adequate access to grocery stores, according to state and federal statistics used by the mapmakers. The tract is about 16 miles south of Hope Covenant House, almost in South Carolina.
This segment of Mecklenburg County has no issues with access to fresh, healthy food, as shown on the new maps.
Another key number shown by the map is what’s called the z-score, the amount by which the combined social determinants in a given area, in this case a census tract, vary from the average in the region of counties. The z-score for the area where Loaves & Fishes placed the new pantry shows that the tract was among the region’s greatest deficiencies in the areas considered.
Locating and fixing such problem areas is the heart of the mapping effort, state officials said.
“No matter what our respective goals — to mitigate the opioid crisis, to ensure our children are healthy, safe and ready to learn, to increase employment or to drive economic growth — it all begins with healthy people,” Dr. Mandy Cohen, DHHS secretary, said in a statement.
Regional comparisons
A measure called the Social Determinants of Health Index combines indicators into three groups, each with equal weight in determining a final score. The individual and overall scores are compared to other counties in the same region, making statewide comparisons unrealistic.
“If you’re a coastal tract in Brunswick, you’re comparing yourself to every county in the state and it loses a lot of its usefulness,” said Matt Simon, a GIS analyst at the public health institute. “It makes more sense to compare it on a region-by-region basis.”
Still, it’s inevitable that users will find their own ways to use the map’s wealth of information, not all of it medical. Want to know the median income in Wake County? It’s $70,620, compared to $31,129 in Bertie County in Northeastern North Carolina.
Interested in the rate of people living below poverty levels in the west side of Lumberton, where Hurricane Matthew ripped up homes, churches and businesses? It’s 54.1 percent, compared to 10.6 percent living below poverty in a tract just west of booming Asheville.
Numbers such as these can suggest projects in the making for public, private and nonprofit interests.
“I think that that’s one way that the tool could be used, to figure out where resources are lacking,” Wallace said. “This is basically a conversation starter.”
The map has roots in a pilot project in which the public health institute combined forces with the Carolinas HealthCare System (now known as Atrium Health) to map a 10-county region including CMC’s own Charlotte campus. Another iteration of it is taking place in Raleigh under the auspices of the John Rex Endowment.
So far, there are no plans or funding to make the state map part of a longitudinal effort, such as the one seen the annual county assessments by the Robert Wood Johnson Foundation.
“We would love to say yes to that,” Wallace said. “We really want to do this long-term.”
Will Cain drove the carcass of a dead calf from Cumberland County to a state lab in Raleigh early this month hoping someone, someday can tell him if chemical pollution harmed it.
Cain raises beef cattle on multiple plots north of the sprawling Chemours chemical factory property south of Fayetteville, including land about two miles away. Like some farmers nearby, he wonders if recently detected chemical pollution from the plant in air, soil or water threatens his livestock or other food raised nearby.
“The consumer has the right to know,” said Cain, who sells cattle to feedlots in corn-rich states such as Kansas to fatten them up before they are slaughtered and their meat readied for market.
Let’s be clear: Aside from a GenX chemical found in one sample of local honey, there is no publicly known evidence that industrial pollution released by Chemours or DuPont, the previous owner, has tainted foods raised nearby.
State officials are still assessing whether testing is needed in the vicinity of company’s 2,150 acres. Developing a means to conduct meaningful tests of food, they stress, would be a complex task that will take time.
For one, they would need to find or develop methods that detect per- or polyfluroalkyl (PFAS) compounds such as what is commonly called GenX in very different types of organisms, potentially from blueberries to swine. State officials also would need solid data on levels at which contamination could pose a risk to people or the environment.
“You can’t just collect samples of a turnip crop or a collard crop in someone’s garden, send it to the lab, get back a range of values, and not be able to tell the public what it means. We want to be able to say whether it’s safe in food or soil or groundwater,” said Michael Scott, Division of Waste Management director for the state Department of Environmental Quality.
Big challenge
Scientists around the world are raising alarms about PFAS chemical contamination because it potentially carries a triple threat. The chemicals are so tough that they don’t break down in nature; they can accumulate in the tissues of people and other living things, including edible plants; and some bring known or suspect health risks.
Because the compounds are soluble in water, they don’t stay in one place either, instead traveling down rivers, through soils and with rain storms.
PFAS chemicals originating from the Chemours site, on the border of Bladen and Cumberland counties, have been found in residential drinking wells three miles away, in rainwater collected at seven miles distance, and many tens of miles away in drinking water drawn from the Cape Fear in and near Wilmington.
A portion of the industrial compound that Chemours operates on some 2,000 acres wedged between the Cape Fear Riiver and NC Route 87, right where Cumberland and Bladen counties meet. Photo credit: Catherine Clabby
So do plants or animals living close by harbor the chemicals too?
“The food is the next frontier,” said N.C. State University scientist Detlef Knappe, one of the small group of researchers who first detected Chemours chemicals in drinking water in this state.
Members of his laboratory have collected some food grown near Chemours but high-confidence testing remains a work in progress, Knappe said.
Signals from afar
Signals exist that food could be a concern.
In Ohio and West Virginia communities exposed to PFAS released by the DuPont plant now owned by Chemours, people who ate locally-grown vegetables had higher blood levels than others who didn’t. (Blood and urine of North Carolinians downstream of Chemours have been collected too but results are not yet known.)
Sampling has detected PFAS compounds in home gardens near PFAS pollution sites abroad and in Minnesota. Small amounts of GenX were found in plants grown very close to a Chemours plant in The Netherlands, for instance.
Researchers at both locations concluded that the detected amounts in the two spots were low enough that people did not need to stop eating food from their gardens in both places.
But you can’t use studies made at one polluted place to determine risks from PFAS contamination in another place, said Deanna Scher, the principal epidemiologist, and James Kelly, a surveillance and assessment manager at Minnesota’s Department of Health.
That’s because contamination levels and other factors differ, just one part of the difficulty of assessing risks from unregulated PFAS that did not undergo rigorous, publicly disclosed health testing before being put to work, they said. “It’s frustrating to have to learn after the fact when the horse is out of the barn and to explain to people we don’t have many of the answers,” Kelly said.
State health officials in North Carolina are testing fish caught in polluted waters near Chemours for PFAS. If comprehensive agricultural testing happens here, it appears that the job will be split between state environmental and agriculture departments.
A memo written by Joe Reardon, assistant commissioner for the N.C. Department of Agriculture and Consumer Services, recommended that DEQ officials focus any sampling they conduct “on commodities that are not entering commerce.”
That’s because the agriculture agency has jurisdiction over marketed agriculture, Reardon said.
Plus, testing without solid information about the risks from contaminants could give inaccurate impressions, said Reardon and agriculture department public affairs director Andrea Ashby.
“We are concerned that the collection of samples without an approved method or toxicological standard to reflect the significance of the findings could create unnecessary consumer anxiety and could negatively affect products’ ability to move in commerce,” Ashby said
Scott, the DEQ director, and NCSU’s Knappe agree that reliable testing and risk assessments standards are needed. Toxicologists with DEQ and the state Department of Health and Human Services are exploring what’s known, Scott said.
State officials until now have depended on a state provisional health goal of 140 parts per trillion as the threshold above which consuming GenX chemicals in drinking water over a lifetime has been posited to pose a health threat.
The US Environmental Protection Agency this summer is expected to release its awaited toxicity assessments for two forms of GenX chemicals, the dimer salt version and another version of Hexafluoropropylene oxide (HFPO), compounds used in the industrial process that Chemours calls GenX.
EPA is also expected to quantify a reference dose, the amount of chemical someone can ingest for a lifetime without anticipating harm.
Waiting
Cain, who drove that calf carcass to the state Rollins Animal Disease Diagnostic Laboratory in Raleigh this month, grew concerned about possible contamination after five calves in his herd of about 200 died during a 10-day span this month, he said.
Cain had sold cows to a close friend, Jeremy Singletary, who lost five calves and adult cows on land about three miles north of Chemours he said he rented about two years ago.
Singletary said a friend froze one dead calf in case it could one day be tested for PFAS contamination.
“I’m not going to sit here and tell you GenX is killing my cows,” Singletary said by phone on Tuesday. “But I do need to know some type of answer.”
Low levels of GenX were recently detected in Robeson County, across the river from Chemours, in its water system and in a swamp about seven miles from the plant. It’s been detected in drinking wells there too.
William Canady, a fifth-generation farmer based in Robeson County, said he has not had mysterious problems with cattle, which he also raises about seven miles from Chemours. But he would like to know if any industrial compounds can be detected in his animals or among the long list of produce he raises for sale, including field corn, sweet corn, soybeans, oats, strawberries and watermelon.
“A lot of people work at that plant. I think the pay can be pretty good,” Canady said. “I just hate to see it doing damage to the community.”
To be cautious, he no longer feeds his cows any of the hay Chemours allowed him to harvest on its property the year before last.
He also wonders if the state has more options than testing commercial livestock to start getting a look at whether PFAS chemical may be tainting meat.
“There are a lot of deer right around that plant,” Canady said. ”They ought to test those deer. And move out from there.”
When it comes to your health, place matters. If you live in a rural county, the bottom-line truth is that you’re less apt to be healthy than if you lived in a more urban one. A couple of recent reports shed some light on both the issues and potential solutions.
According to the 2018 County Health Rankings, published by the Robert Wood Johnson Foundation in partnership with the University of Wisconsin Population Health Institute, rural counties continue to lag behind more urbanized ones in factors that play a critical role in a community’s overall health. These include child poverty, low-birthweight babies and teen birth rate.
But rural communities have within their DNA the resources to rise to these challenges.
In another report, titled “Exploring Strategies to Improve Health and Equity in Rural Communities,” researchers at the University of Chicago’s NORC Walsh Center write that while much of the research exploring rural health issues in the U.S. focuses on disparities – increased health risks “related to geographic, socioeconomic, environmental and other factors” – seldom is attention paid to the strengths and assets within these communities that can be, and often are, deployed to improve health.
These communities’ greatest assets, the researchers assert, are their people: “Commonly reported individual assets include civic and community engagement in the form of volunteerism, strong entrepreneurship, and the resilience and adaptive capacities of rural residents.”
The County Health Rankings report is a call to action. It petitions community “changemakers” to explore the data to better understand the nature of the challenges, and to then more fully leverage assets within the community to address them, implementing strategies that will allow every community member to lead the healthiest life possible.
To advance this initiative, the County Health Rankings & Roadmaps program sends coaches out to assist individual communities.
“We’ve been partnering with the National Association of Counties for the past two years on the Rural Impact County Challenge, working with counties who bring teams together to think about opportunities to take action addressing children in poverty,” says Aliana Havrilla, one of those coaches. “But in my experience, it’s become a much broader conversation about opportunities and assets that exist at the local level.”
Slow recovery
The County Health Rankings underscore the primary role poverty plays in health outcomes and indicate that while child-poverty rates are declining, they remain at levels higher than before the recession.
“In the wake of the Great Recession, rates of children in poverty stayed high through 2012 and, despite declines in recent years, remain higher than the pre-recession era,” says Anne Roubal, a population health analyst for the Rankings & Roadmaps program.
Rates of recovery, she stresses, vary by place and race. “In general, child-poverty rates have not bounced back in many rural counties or those with a greater share of people of color.”
Rural counties continue to have the highest child poverty rates (23.2 percent) followed by large urban metro (21.2 percent), smaller metro (20.5 percent) and suburban counties (14.5 percent).
The County Health Rankings authors write that poverty limits opportunities and increases the likelihood of poor health. Children living in poverty are less likely to have access to quality schools and have fewer chances to prepare for living-wage jobs leading to upward economic mobility and good health.
“Children in poverty is an upstream measure that assesses both current and future health risk,” they write. “Recent data on poverty show that rates among children and youth are at least 1.5 times higher than rates among adults aged 18 and older.”
Disparity among neighbors
Health outcomes in the County Health Rankings are measured by how long people live and how healthy they feel. Length of life is measured by premature death – deaths that occur before individuals reach their statistical life expectancy. Quality of life is measured by the percentage of days people report poor or fair health, the percentage who report physically and mentally unhealthy days within the past 30 days and the percentage of low-birth-weight babies.
The disparity between rural and urban counties in these measures and others is often stark.
Take, for example, the North Carolina counties of Wake and Robeson. Wake County, where Raleigh, the state capital, is located, is part of a thriving metropolitan area with more than 2 million residents. It ranks first in the state in the report’s health outcomes.
Robeson County, an hour-and-a-half drive to the southeast, is largely rural. The largest city, Lumberton, has a population of about 21,000. It’s ethnically diverse, roughly 40 percent Native American, 30 percent white and 25 percent black. Robeson ranks last, 100th, in health outcomes in the state.
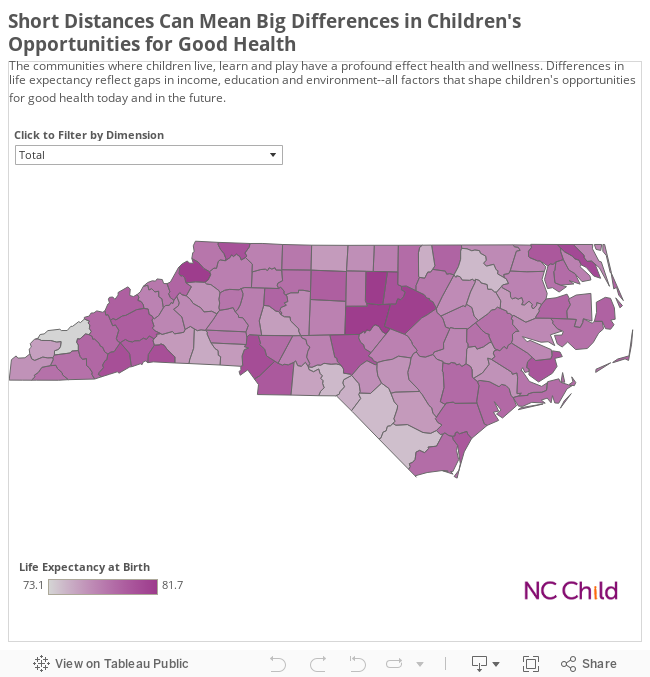
Data, visualization courtesy: NC Child
County Health Rankings data indicate that Robeson County residents reported more than twice as many days being in poor or fair health than Wake County residents (29 percent vs. 13 percent). Nearly twice as many Robeson County residents reported physically unhealthy days within the past 30 days (5.4 percent vs. 2.9 percent) and more reported mentally unhealthy days (5.4 percent vs. 3.6 percent). A Robeson County adult is also much more likely to be obese (39 percent vs. 23 percent).
The data further indicate that there are more than two and a half times as many premature deaths each year in Robeson County than in Wake County.
Now consider poverty. Its correlation with poor health outcomes is underscored in the contrast between these two counties.
Robeson County has the highest rate of poverty in the state, among the highest in the country. Nearly a third of all residents live below the federal poverty level (in 2017, $24,600 for a family of four); nearly half of all children live in poverty. Almost twice as many Robeson residents as Wake residents are unemployed (7.9 percent vs. 4.2 percent) and twice as many are uninsured (20 percent vs. 10 percent).
Lumberton, the county seat of Robeson County, is 100 miles and a world of difference from Raleigh.
Local connections
“Things are improving,” Anne Roubal says of the national outlook – slowly. “Starting in 2008, we saw a jump in poverty pretty much everywhere and that trend continued for three years.” Things then began to improve, but not as quickly as they’d gone into decline. “We’re still not back to where we were in 2006 and 2007.”
The resources needed to recover and to build healthier communities are found in rural America. Health care institutions in many rural regions are taking innovative approaches to meeting their communities’ needs. In Robeson County, the local hospital, Southeastern Health, is tackling its community’s health care issues by remaining independent and offering a broad range of care under one roof.
But it’s often individuals who step forward. According to the NORC Walsh Center report, “participation in community life in rural areas often stems from strong individual relationships and connections that people form with one another.” Such connections “lead people to participate in volunteering, community organizing and coalition building.
“One thing I really appreciate about rural communities is that they have a culture of such strong collaboration,” Aliana Havrilla says. “Sometimes, it’s everybody knows everybody because many people wear many hats. There’s also often just that tight-knit community feel … a strong asset-based collaborative approach that they’re bringing to this work addressing complex issues.”
When it comes to health care, one of the biggest problems faced by rural residents often is finding a doctor, dentists or other practitioner near home.
A bill unveiled in the waning days of the annual legislative work session seeks to find ways to incentivize more medical providers to settle – and stay – in rural North Carolina.
“If individuals practice, or learn or are educated in rural areas, they tend to stay in rural areas,” Rep. Greg Murphy (R-Greenville) told his fellow lawmakers this week as he moved a bill that will study what it takes to get and keep health care providers in rural burgs.
Lawmakers spent last winter on two different committees which were dedicated to examining health care workforce issues throughout North Carolina. One of those committees sought ideas on the best ways to improve health care access in rural parts of the state, the other, headed by Murphy, looked at how to help induce physicians to practice in rural areas.
One way to do that is to create more training opportunities in rural areas themselves. To that end, the bill orders the Department of Health and Human Services to identify which rural hospitals could become teaching facilities and figure out what they’d need to become successful.
“Take Ahoskie, for example, it is a very rural hospital, has a 120 bed system,” said Murphy. “It’s putting family practitioners, family practice residents to rotate out in those areas, it’s possible to put internal medicine residents there … just a rotational thing.”
But making the conversion to instruction is no easy task, said Southeastern Health CEO Joann Anderson. Her Lumberton-based hospital partnered with Campbell University to start a medical residency program which will graduate its first students this month. Four of the primary care residents signed up to stay in Lumberton, another two will move to rural Western North Carolina. The program has also recruited education slots for family doctors and emergency medicine.
Sponsored
“This year, we had six slots for emergency medicine, we had more than 600 applicants,” she told lawmakers this March when the rural health care access committee visited Columbus County.
But to do this is expensive. Anderson described the dollars spent on startup costs, enhanced salaries to attract faculty and students, and equipment.
“It was a little over $11 million for this year,” Anderson said. “The cost of that was the salaries for each of the residents, faculty costs, the location, the space that we had to provide for them, all the equipment they had to have. For example, we had to buy three ultrasound machines for them to use. Each costs thousands of dollars.”
The bill also instructs DHHS to rejigger its North Carolina State Loan Repayment Program to help people practicing in rural areas shed their debt, with an eye toward recruiting new providers to small towns and getting them to stay there.
Dentist credentialing gets nod
And, at the last minute, lawmakers inserted a provision to make it easier for dentists from the neighboring states of Virginia, Tennessee, Georgia and South Carolina to become licensed in North Carolina.
In the past, dentists from other states have had to jump through multiple hoops to obtain a license to practice here. Until now, North Carolina has only accepted dentists who have passed a credentialing exam that’s accepted in only seven other places: Alabama, Louisiana, Puerto Rico, the US Virgin Islands, West Virginia, Arkansas and Utah. Dentists from states other than those have had to submit to a recredentialing process that can take months and cost thousands of dollars.
In some quarters, this has been seen as a block to getting more dentists into North Carolina, which has historically had fewer dentists per capita than most other states. Three counties in the state have no dentist and the state consistently ranks 47th among the 50 states in terms of dentist-to-population ratio.
Map caption: North Carolina has about 4.7 dentists for every 10,000 people. Nationally, the ratio is closer to about 6.2 dentists for every 10,000 people.
“That certainly may have an impact on addressing the dental workforce capacity in counties adjoining the neighbor states, particularly in our more rural counties,” wrote Lewis Lampiris, who trains students in community dentistry at UNC-Chapel Hill’s dental school.
Lampiris noted another important change, namely loosening restrictions on dentists who receive these licenses “by credential.” Currently, dentists licensed by credential have to choose only North Carolina as a location for practice; this has limited the ability for dentists in towns along North Carolina borders to open up a satellite office across state lines.
The bill removes that restriction.
The Senate passed the bill with little debate. But Sen. Erica Smith (D-Jackson) said the bill falls short in one important way.
“The elephant in the room and in this bill is the lack of opportunity to study Medicaid expansion,” Smith said.
“How do you improve rural health care?” she asked. “You expand [Medicaid].”
Historically, the residents of rural Robeson County have relied heavily on the Southeastern Health Emergency Department for much of their medical care, even for non-emergent issues such as sore throats and sprains.
The hospital, located in the county seat of Lumberton, has about 90,000 ED visits per year, according to Southeastern Health CEO Joann Anderson.
The front desk of Southeastern Health’s Walmart urgent care. It’s is a three-room clinic that serves as a place where patients can get their non-emergency health needs taken care of quickly without going to the hospital’s Emergency Department. Prices are clearly listed on the wall at the entrance. Photo credit: Taylor Knopf
“If you ask a lot of people in Robeson County who their primary care provider is, they are going to give you an emergency department physician name,” Anderson told the legislative Committee on Access to Healthcare in Rural North Carolina earlier this year when lawmakers traveled to Columbus County to meet with hospital CEOs and rural health providers.
ED overuse is not just a problem in Robeson County. The hospital CEOs from Columbus and Scotland Counties also told state lawmakers about similar issues in their communities. All these health care CEOs want patients to instead use urgent care clinics for non-emergency conditions such as the flu, a urinary tract infection or minor cuts.
“There’s really no reason for them to be there,” Anderson said. “So how do we make that happen?”
A price list for common procedures and visits to the Walmart/ Southeastern Health clinic, complete with ICD-10 codes. Photo credit: Taylor Knopf
The answer has come with making urgent care clinics easier to get to than the hospital. In Lumberton, that means there’s an urgent care right inside the entrance of the local Walmart.
Overused
All the CEOs said there’s several reasons why it’s hard to break the habit of turning to the emergency room for everything. For starters, there are uninsured people who use emergency departments because they know they can’t be turned away. That’s because once a patient sets foot inside an emergency room, providers there are obligated by federal law and other rules to treat and stabilize them.
In Robeson County, Anderson said she doesn’t know exactly how much money her ED loses each year, but said Southeastern Health’s finances have little room for error.
“The operating margin for the last five years has been about 1.3 percent, which is low,” she said. “Last year we actually lost money.”
Southeastern Health looks to its walk-in urgent care clinics – including the Walmart location – to take the pressure of the ED. Anderson said the Walmart site is “unique” and is one of Southeastern Health’s busiest.
Prices are posted on the wall, so patients know exactly how much they are going to spend. And since it’s located inside a major shopping destination, many customers see it. Plus, Walmart’s pharmacy is located nearby, so patients can get their prescriptions filled immediately.
Inside Walmart
Will Von Taborsky works at the Walmart vision center just next to Southeastern Health’s urgent care clinic. He finds the clinic to be very helpful for his family and his boy scout troop.
Will Von Taborsky is the Walmart vision center manager which is located right next to Southeastern Health’s urgent care clinic. He said his family will frequently use the clinic for colds and other non-emergency health needs. He said it’s also a great place to get a quick sports physical for a decent rate. Photo credit: Taylor Knopf
“We’ve used it as a family for personal things like colds and flus and shots and that type of thing,” he said. “But the other thing I find it very convenient for, hanging out with young people in the community, is sports physicals or summer camp physicals.”
He’s the scout master and will tell parents the walk-in clinic is a “quick, easy and inexpensive” place to get that last-minute physical. Those are only $25.
If you don’t have health insurance, a sick visit at the Walmart clinic is $65.
Brooke Grooms is a nurse practitioner there. She said compared to other urgent cares, the Walmart location is a “fast-paced, ‘street and treat’ kind of clinic.”
It only has one exam room.
“They are in and out within 15 minutes,” she said. “We don’t see complex issues here, just sinus infections, colds, flu… There are times where I’ll do more complex things like suturing, abscess drainage, but that’s only if I don’t have a line.”
She sends those needing more advanced care to the Southeastern Health’s “mall clinic,” which has four patient exam rooms, more staff, and the ability to set fractures and perform X-rays.
Southeastern Health’s Walmart urgent care is a three-room clinic that serves as a place where patients can get their non-emergency health needs taken care of quickly without going to the hospital’s Emergency Department. Photo credit: Taylor Knopf
“If we see it’s something where there’s chest pain, shortness of breath, and high blood pressure, they go straight to the ER,” Grooms said. “If they look bad enough, we can call the ambulance.”
She said she’ll see some of the same patients over and over.
“Some are regular Walmart shoppers,” she said. “We are the only Walmart with a clinic. People walk by and see us.”
Grooms emphasized that she is not a primary care provider, even though many patients try to treat her as such. She can give prescriptions refills on a limited basis, because she said it can be difficult to get in to see a primary care provider.
Her mother was a primary care doctor in Robeson County for 27 years, and Grooms said her mom frequently saw her patients the same day they called. But that’s not the case anymore.
Sponsored
Grooms said she believed the urgent care clinics take the load off primary care offices more than the Emergency Department.
“I use to be an ER nurse. It was bad. We had 13-15 hour waits, and a lot of this county is unemployed,” she said. “With unemployment comes no insurance. The only place in town that will see you regardless of anything is the ER.”
Across from the hospital
Another way Southeastern has sought to divert patients on their way to the emergency room is by placing another urgent care clinic right across the street from Southeastern Health’s hospital emergency department.
The “health mall” across the street from the Southeast Health’s main hospital is a place where hospital leaders are encouraging patients with less emergent problems to get seen. Photo credit: Taylor Knopf
Barry Graham is a physician assistant there in the “health mall.” He said it’s difficult to say how many patients come to the urgent care instead of the ED. Some people definitely walk into his clinic who should be getting emergency care.
The health mall is in a strip mall next to a JC Penny and has a variety of providers and services. Within the health mall, there is an express lab, an urgent care, a pharmacy, a surgical center, weight loss center, and a diabetes community center.
The health mall urgent care clinic is open Monday through Friday from 8 a.m. to 5 p.m., as well as some weekend hours and Graham said the clinic is in the process of expanding to evening hours. He sees about 30 patients a day, which is more than most primary care providers will see in the same time period.
But Graham agreed with Grooms, saying his clinic likely takes more pressure off of primary care physicians with busy offices than the ED.
“I mean, they try to see walk-ins but, but you know, especially as it gets later on in the day, it’s hard to have a walk-in,” he said. “They feel comfortable having folks come see us.”
This week, a group of UNC-Chapel Hill students piled into their vehicles and headed off for spring break. But instead of heading for the coast or mountains, their first stop was the Robeson County city of Lumberton.
Close to two dozen students opted to spend their vacation taking a service-learning course aimed at helping communities affected by Hurricane Matthew. UNC partnered with churches and local health organizations to offer two free health clinics – the first on Tuesday in Robeson County and the second on Thursday in Columbus County.
“I’ve lived here all my life, but didn’t know a lot about the rural population,” said UNC-Chapel Hill freshman Alexis Payton from Raleigh. “I knew there was a disparity between rural and urban counties. I’m just getting to learn more about that.”
Inside the health clinic on Tuesday, medical stations lined three rooms of a former Lumberton ammunition factory. It serves as a temporary site for Robeson County Church and Community Center displaced by the hurricane.
At intake tables, community members filled out basic forms with age and gender but no identifying information. Student volunteers asked for some brief medical history such as tobacco use, diabetes, high blood pressure and asthma.
From there, patients could visit the nutrition table, get their vitals taken, or have an eye exam or HIV screening. Multiple stations offered information about free local programs, including some for new or expectant mothers or people with diabetes. Volunteers at a health care navigation table showed Robeson residents available services and helped them schedule appointments.
Many stopped at the mental health station where two professionals screened for depression and substance abuse. Often people wanted to share their experiences of Hurricane Matthew.
One woman confided in volunteer Richard Unkiewicz, a psychologist from Goldsboro’s Cherry Hospital, about her husband’s cocaine use. Unkiewicz said she is stressed and doesn’t know what to do, so he wrote her a referral to get some help.
“We try to get them to tell us a little bit about themselves,” he explained. “If they don’t want to talk, that’s fine. Usually, more cases than not, they will start talking. They start revealing things, but they have to connect with you.”
Despite the rain Tuesday morning, clinic volunteers saw more than 50 patients that afternoon. Organizers decided to extend the Lumberton clinic a second day and handed out flyers at motels where many are still homeless as a result of the hurricane.
Matthew’s destruction
When Matthew raged through Lumberton in October, about 20 inches of rain filled the sanctuary of Branch Street United Methodist Church.
Carlotta Winston, health promotion specialist with Southeastern Health in Lumberton, explained healthy eating and nutrition to Robeson County residents who visited the free health clinic Tuesday. Photo credit: Taylor Knopf
The church lost everything except three pews and a piano. A month went by before the congregation could even hold a service in its adjoining fellowship hall. Three out of 60 church members were displaced from their homes due to flooding.
“We were on an island, you go this way hoping you could get home, you would have to turn around and go another way because of the floods and bridges washed out,” said Rev. Douglas Locklear.
“We’ve never seen anything like this. For weeks it looked like you were on the shore lines, so much pure white sand,” he continued.
Locklear said that without flood insurance, it will take about $150,000 to repair the damage to his sanctuary. Church members have worked three nights a week on repairs.
Forty-year Robeson County resident Sheila Hammonds took advantage of the Lumberton health clinic Tuesday. She and her two children have been living with her sister since the hurricane and she said she considers herself lucky not to be in a shelter or motel. The first floor of Hammonds’ apartment complex flooded, and she’s been told by management she can hopefully return home late this spring.
Hammonds works at the Church and Community Center where donations are received and redistributed.
“We are trying to help people get back on their feet,” she said. “It may not be as good as it was before, but at least they have somewhere in the community they can come and receive care.”
Branch Street UMC partnered with Christ United Methodist in Chapel Hill which also sent volunteers with the UNC clinic team. Christ United sends volunteers to the area every few months.
“The idea is you keep coming down,” said church volunteer Scottie Pitner. “Don’t forget people, because they feel forgotten.”
Locklear said he and his community appreciate the students and volunteers who set up the health screenings.
“For UNC-Chapel Hill to come and do this health clinic means so much to us, especially our elders who live on a fixed income,” he said. “They have to make a choice every month to get their blood pressure or diabetes checked or pay their light bill.”
Local partners
Students and staff from UNC-Pembroke were not on spring break, yet came by to lend a hand.
Christina Tunstall, nursing student at UNC-Pembroke, took blood pressure at the free clinic Tuesday for residents of Robeson County affected by Hurricane Matthew. Photo credit: Taylor Knopf
Jennifer Twaddell, UNC-Pembroke Interim chair of nursing, said Pembroke is a name community members recognize and acts as a bridge into the community. So when UNC-Chapel Hill asked Pembroke to partner in the clinics, she couldn’t say no.
“These guys are doing this out of the goodness of their heart, they are not getting credit for this,” she said of her students working the clinic.
Christina Tunstall is a second year nursing student at UNC-Pembroke who volunteered Tuesday taking blood pressures at the clinic. She said all the people she checked ran high.
“A lot of people specifically in this area may not have the finances or insurance to go to the community hospital or clinic where they sometimes charge for things like blood pressure or blood glucose checks,” she added. “So it’s really important for people to have a place to go to for simple screenings.”
Tunstall lives in Fayetteville and her husband serves on Fort Bragg. Being from a military family and moving a lot, she said she didn’t always connect with the residents around her. But she is glad to connect with the community members in Robeson County.
“It’s awesome to go to a school that places a lot of importance on serving the local community,” Tunstall said.
When Tona Jacobs, the vibrant principal of Pembroke Elementary School, fainted twice at work five years ago, she figured she was just weak from giving blood earlier that day.
But no.
After her staff insisted she take an ambulance to a local hospital, an ultrasound revealed waxy plaque narrowing the arteries in her carotid arteries, connecting her brain to the rest of her body. That’s serious business, a symptom of atherosclerosis, which can lead to stroke, heart attack or death.
Pembroke Elementary School principal Tona M. Jacobs (left) and UNC-Chapel Hill researcher Jada Lyn Brooks outside the school’s front office. Photo credit: Catherine Clabby
“That was a scare. I may not have known that until it was too late. I thought I was healthy,” said Jacobs, 56, a health-conscious member of the Lumbee Indian tribe clustered in and near Robeson County.
As it turns out, simply being an American Indian puts Jacobs and other Lumbee woman at increased risk of developing cardiovascular disease, or even prematurely dying from it.
Death rates from the disorder among Indian women in southeastern North Carolina are among the highest in the country, said Jada Lynn Brooks, an assistant professor of nursing at UNC-Chapel Hill.
Brooks, who is also Lumbee, wants to find out why.
Brooks suspects one problem could be people’s environmental exposures, possibly from minute particles emitted from the tail pipes of the gas- and diesel-powered vehicles traveling up and down Interstate 95 in Robeson County.
Psychological factors could be in play, too.
If Brooks cracks the mystery, she wants to then help reduce the scourge, something that could extend the lives of Lubee woman.
“I’m always looking for solutions to a problem,” said Brooks, who landed a $741,355 National Institute of Environmental Health Sciences grant and help from more senior scientists at UNC to tackle her query.
Loyal to home
Brooks, who is 37, grew up in the Lumbee Prospect Community, not far from UNC-Pembroke, where she enrolled to study science straight out of high school.
When she peppered a pediatrician she shadowed at that time about root causes of the many asthma cases he saw among patients, he recommended she get graduate training in public health to help her find out. She did, at the elite Gillings School of Global Public Health at UNC Chapel Hill.
Tributes to Lumbee heritage are not hard to find in Robeson County. This artwork hangs inside UNC Pembroke’s Thomas Family Center for Entrepreneurship, where Jada Lynn Brooks has an office. Photo credit: Catherine Clabby
As her interests in clinical care and the bigger picture grew, she earned a second bachelor’s in nursing and then a doctorate, too, at Duke University, working with premature babies back home in Robeson County and, eventually, having three children of her own.
Already a veteran health researcher, Brooks has worked on projects to improve mammogram screening rates among minorities, expand access to smoking-reduction program for similar populations, and better understand the challenges faced by mothers whose babies are born premature.
“All of my research has been aimed at understanding health disparities and trying to figure out what we can do to address them,” Brooks said.
There’s plenty to do. Significant numbers of Lumbee people historically have grappled with poverty, high rates of obesity and chronic illness—diabetes and depression among them—at rates higher than white North Carolinians. As recently as 10 years ago, Lumbee people were, on average, less likely to have health insurance and access to affordable health care.
But the statistics don’t fully explain the disproportionate burden of disease among Lumbee women, said Brooks, who will recruit 120 tribal women ages 28 to 45 to help her find answers.
The project aims to take blood samples from each woman and use EPA air pollution measurements to look for any correlation between a woman’s exposure to particulates in the air and biomarkers in blood associated with atherosclerosis. In addition, Brooks and her research team want to explore whether a woman’s positivity, or lack there of, is associated with higher or lower inflammation markers.
The women will be queried about how frequently they feel interest in their lives. She’ll also ask about love and pride, and how often they feel contempt, embarrassment and guilt.
To help her conduct studies that are culturally appropriate, Brooks has solicited advice from leaders within the community, including Jacobs, the elementary school principal.
Sponsored
Those advisors have nudged Brooks to inquire about religious beliefs and practices when probing mood, since so many Christian churches steeples — mostly Methodist and Baptist — are found in Lumbee communities.
During a phone meeting earlier this week, some members also questioned her closely about what she planned to do with the blood samples after her study is finished, about five years from now. Brooks said she may destroy them, though she is not sure. No matter what the plan, her consent form for the study will put research subjects in charge of how the samples are used.
Dr. Martin Luther Brooks opened his general medical practice in Robeson County in 1958 and still practices there. A Lumbee, he has worked to improve preventative treatment among his patients and is among the community advisors to Jada Lynn Brooks’ latest research project. Photo courtesy of Dr. Brooks.
“You have to be careful with consent so that people know what they are giving permission for signing up for,” Brooks said.
A link in a chain
Martin Luther Brooks, a Lumbee physician with a general medicine practice in Pembroke since 1958, is also on Jada Lynn Brooks’ advisory team.
He has long observed gaps in the medical care Lumbee women receive. One example from early in his practice was his discovery that there were no statistics on cervical cancer among North Carolina Indian women in state records.
They were not immune. They were just not getting the pap smears that detect that cancer, a deficit he worked hard to reverse, despite opposition from his patients due to modesty, lack of funds and ignorance about the risks they faced.
“We’re still aren’t getting women enough basic fundamental information about their own health. Self care has to predate health care. If it does not, when health care arrives, it gets there too late,” said Brooks, who is not related to the UNC researcher.
Jacobs, the principal, says she thinks wider cultural forces could play a role in Lumbee women’s higher rates of cardiovascular disease. Possibly like women in many communities, they focus more on others – parents, children and spouses – than they do on themselves.
“We don’t focus on ourselves. You are considered the backbone. You can’t be sick,” Jacobs said. “You have to take care of all these other things.”
The cardiovascular study that Jada Lynn Brooks is launching could help women understand why they must work harder to look after themselves too, Jacobs said.
“There is so much that could come from this study — to help people my age but also to better educate our children,” she said. “We need to put things in place to help our children.”
After police shot and killed a Charlotte man who was deaf last year, some North Carolina lawmakers want to take a closer look at law enforcement mental health and disability training.
House Bill 591 would direct the state Departments of Justice and Public Safety to study different types of training available for officers to improve their traffic stop interactions with individuals with disabilities. The bill, sponsored by Rep. Charles Graham (D-Lumberton), passed through the House Health committee last week.
Rep. Charles Graham (R-Lumberton)
Graham worked with students with special needs in Robeson County for 31 years and said many of his students went on to receive a driver’s license. He cited oppositional defiance disorder, traumatic brain injury and post-traumatic stress disorder as just a few of the issues that affect a person’s ability to interact with a police officer.
“Just because you become a certain age to have a driver’s license doesn’t mean that diagnosis disappears,” he said. “A person always carries that diagnosis.”
“Not all drivers have normal functional and cognitive abilities,” Graham said. “Although they have a driver’s license — and they are entitled to have the driver’s license — they don’t have what we consider to be normal behavioral interactions.”
That phenomenon was in evidence during another incident in Charlotte last year, where a man acting erratically was shot and killed by police; it was later discovered that he had a traumatic brain injury.
Raleigh CIT officer Wendy Clark and counselor Benny Langdon demonstrate how to handle an intoxicated, combative man during the Wake County CIT training in 2013. Photo credit: Rose Hoban
During last week’s committee meeting, Rep. Cynthia Ball (D-Raleigh) spoke in support of Graham’s bill, adding that she sponsored legislation that would create a designation on driver’s licenses to identify deaf and hearing impaired drivers. House Bill 84 has already passed the House and is moving through the Senate.
Rep. Jay Adams (R-Hickory) asked if lawmakers should be studying “at what point a person is not eligible for a driver’s license […] Are there people out there who are licensed to drive that are virtually going to be impossible to deal with?”
Graham said that is not within the scope of this study bill. Its goal is to determine whether law enforcement needs a certain level of mental health and disability training, and if so, what should that be.
“I don’t think we can put a label on a person and say, ‘because you have PTSD, you’re not eligible for a driver’s license,'” Graham said. “I don’t want to imply that’s what this study is about.”
“We have people that go into law enforcement with a high school diploma,” he added. “They have no knowledge of what PTSD is. The have no knowledge of what some of these diagnosis might carry.”
All law enforcement officers have a mental health awareness course during basic training. About 45 percent go through additional Crisis Intervention Training (CIT), a more robust course available across the state for any interested officers. It teaches them skills such as how to de-escalate a situation.
By the end of last year, 9,536 North Carolina law enforcement officers completed the CIT program out of about 21,000 full-time officers, according to the N.C. Department of Health and Human Services.
Rep. Beverly Boswell (R-Kill Devil Hills)
The North Carolina chapter of the National Alliance on Mental Illness helps revise the curriculum for the CIT program every few years. NAMI NC Executive Director Jack Register said his organization always supports study legislation like House Bill 591, especially because CIT is the only real training in the state. So exploring options is welcome.
Rep. Beverly Boswell (R- Kill Devil Hills) was the only lawmaker in the committee to vote against the bill on Tuesday.
“When a police officer pulls you over, he asks that you follow simple commands,” Boswell said. “So is that the issue? Or are we going to make the police officers a medical provider? Because that’s a very thin line.
“All drivers have to obey the same rules and regulations” she added. “So if they are unable to follow the commands of a police officer how can they have a valid driver’s license?”
Matthew Herr, policy analyst with Disability Rights, spoke in support of the bill. He said when it comes to someone with autism, for example, “they may be able to follow commands but it may take them longer, or they may have some informational processing limitations that slows down their reaction.”
He pointed out that there is already a medical review process in place at the North Carolina Division of Motor Vehicles.
But Herr noted there is not a consensus among disability advocates about how law enforcement should approach these individuals, which is why he thinks a study is so needed.
“When we say people with disabilities, it’s deceptively complex term,” he said. “The best practices for dealing with a person with autism may be different than the best practices for dealing with a person with severe anxiety.”
State environmental regulators are investigating how to stop the release of air emissions carrying compounds related to GenX from the Chemours manufacturing site in Bladen County that chemical giant DuPont ran for decades.
That’s because those emissions may be contributing to contamination detected in recent months in private drinking wells close to the facility, as well as in public drinking water systems downstream that draw from the Cape Fear River.
Department of Environmental Quality air specialists are researching techniques that could capture emissions of a long list of unregulated perfluorinated compounds, known as PFAS, from multiple smokestacks on the 2,200-acre site, said agency air quality division director Mike Abraczinskas.
Data that DEQ requested from Chemours suggests practically no GenX was released into the atmosphere from 2012 to 2016. But other unregulated compounds have been emitted, including one discharged at levels reaching 75,000 pounds in one year.
DEQ and the state Department of Health and Human Services will host a third community information session on its well testing program near Chemours at 6 pm Thursday, Dec. 14, at Gray’s Creek High School auditorium in Hope Mills.
Figuring out whether any of those compounds pose risks to people could take a very long time. So in the shorter term, DEQ wants to guide Chemours on what pollution controls the company can use to stop the emissions, Abraczinskas said during an interview with NC Health News last week.
“We’re asking: how can we eliminate or destroy all of these before they are emitted,” he said.
Airborne concerns
It could be that air emissions that regulators don’t yet understand might be the culprit behind why Genx has been detected in private wells farther than expected from the Fayetteville Works manufacturing site.
For one thing, the chemical was detected in levels high above North Carolina’s established health goal of 140 parts per trillion in wells on land across the expanse of the Cape Fear River. Normally a river of that size would be a barrier to polluted groundwater moving from one place to another.
Meteorological data collected from 1998 to 2017 at Fayetteville Regional Airport and analyzed by DEQ shows wind patterns that cross the Chemours site. Those breezes would likely have moved any emissions to the northeast and southwest of the industrial property, and over locations where well tests are now turning up positive for GenX.
Chemours emission estimates created by DEQ with a widely accepted computer model suggests only very small amounts of GenX and very closely related compounds have been emitted from the facility.
The state Department of Environmental Quality wants to confirm this Chemours estimate of GenX and similar compound emissions with stack testing the company will perform with equipment and procedures DEQ endorses. Source: DEQ
But it’s also known that one of these chemicals, known as C3 dimer acid fluoride, can convert to GenX after contact with water. What’s not known is whether any of that compound released from the Chemours facility was transformed this way, Abraczinskas said.
“If you emit it as a gas, how quickly will it convert to GenX?” Abraczinskas asked. “Does it happen in the presence of water vapor, with rain, or does it have to deposit in a puddle? We’re asking universities, the EPA and the company. We don’t have answers yet.”
To confirm the Chemours estimates, the state is having the company sample for any GenX that gets past the smokestack scrubbing equipment during normal operations.
Meteorological data from Fayetteville Regional Airport has helped state regulators predict where air emissions from Chemours are most likely to be found. Source: DEQ
Last month DEQ Secretary Michael Regan moved to revoke a significant portion of Chemours’ permit to discharge wastewater into the Cape Fear after the company failed to report a spill that elevated its GenX discharges into the Cape Fear River. DEQ asked the State Bureau of Investigation to investigate if Chemours broke any criminal law by not disclosing the release.
New players
Also of interest is a long list of related compounds the facility released into the air between 2012 and 2016, data that the company recently collated for DEQ. One of particular note is hexafluoropropylene oxide (HFPO), whose release reached 72,500 pounds in 2015 and 42,119 pounds in 2016.
DEQ leaders Michael Scott with the waste management division, Linda Culpepper with water resources and Mike Abraczinskas with air quality speak with state Rep. Pricey Harrison, (D-Greensboro), in blue, after a meeting of the House Special Select Committee on North Carolina River Quality last week. Source: DEQ
“The question is what does that stuff do?” Abraczinskas said of the HFPO emissions. “We know it’s an essential building block to a lot of things they make. Does it have the potential to form GenX in any way? We’re trying to find out.”
A DuPont brochure says HFPO can be used to produce perfluorinated vinyl ethers which are used in the production of commercial fluoropolymers, which are used in thousands of products, including non-stick coatings such as Teflon.
Sponsored
Last summer, a Chemours representative told state and locals officials that GenX detected in the Cape Fear was a byproduct of one of these vinyl ether processes. But he noted that particular process was exempted from an EPA order that Chemours not release GenX into the environment due to potential health concerns.
Eager for a fix
State Rep. Ted Davis (R-Wilmington) last week said he does not agree with some people who are calling for Chemours to be shut down. At the same time, he said steps must be taken to ensure that people are not exposed to dangerous industrial chemicals originating there.
Rep. Ted Davis, Jr. (R-Wilmington)
“You’ve got to weigh the safety of the people with the benefits of that industry being here,” said Davis who co-chairs a House committee on Clean Rivers, created after news of GenX contamination broke. “To me, it makes sense to let the company operate but take that stuff elsewhere.”
Neighbors to the Chemours compound are carefully watching everything state officials are doing to eliminate and, eventually, clean up any pollution close to their homes.
Many are alarmed by the results of well tests that DEQ Assistant Secretary Sheila Holman reported last week during a meeting of the House Select Committee on River Quality, which Davis co-chairs.
In a first round of testing starting in September, 51 out of 141 wells had concentrations of GenX above the state’s provisional health goal; 35 had no GenX detected. A second round begun in October expanded sampling to 450 properties within one mile of Chemours’ property line. As of last week, 34 out of 107 wells sampled had concentrations of GenX above the state’s health goal; only 25 showed no GenX.
Chemours, state officials and Bladen and Cumberland County officials have met to discuss how to best get new water supplies into homes whose wells have GenX exceeding the state health goal.
Mike Watters, a founder of Grays Creek Residents United Against GenX in our Wells and Rivers, says Chemours should pay to connect residents to municipal water supplies and compensate them for the equivalent of any property value they’ve lost.
In addition to exposure via water, Watters wondered what air emissions may have done to soils, home vegetable gardens and crops raised to feed livestock. He was disheartened by news Monday that GenX has been detected in food: in honey harvested from a beehive in Robeson County.
Long-term health monitoring of people who live near the plant is going to be vital, he argued.
Members of a committee examining access to care for people in rural North Carolina hit the road last week, bringing lobbyists, lawmakers and legislative staff to Columbus County, two hours southeast of Raleigh, for a hearing.
“Whiteville is a very unique place in that it is a very rural community, still has a very traditional rural-based economy, but it is a community that still is somewhat vibrant,” said committee co-chair Rep. David Lewis (R-Dunn). “So we thought this would let us see the challenges that are faced by even a more successful or more wealthy community. Certainly, if this hospital faces them then one in a poorer community will have more challenges.”
Committee members heard formal presentations from the head of hospitals in Columbus, Robeson and Scotland counties, all facilities serving primarily rural populations. The three counties consistently rank at the very bottom of annual county health rankings, and each has some of the highest rates of poverty in the state.
The three hospital CEOs talked through their telehealth initiatives, the challenges of recruiting and keeping health care providers, and emergency departments jammed with behavioral health patients.
The presentations were followed by a relatively freewheeling lunchtime discussion with the hospital leaders, something usually not allowed for in an ordinary hearing. The CEOs discussed what they need to survive in an increasingly consolidated and competitive health care marketplace marked by non-paying and uninsured patients, decreasing reimbursements from commercial insurance plans, and uncertainty facing governmental payers such as Medicaid and Medicare.
“We’re serious about trying to make a difference and improve access to health care,” Lewis told the CEOs.
Call a doctor
Each hospital leaders described their use of telehealth services to fill some of the gaps in care created by personnel shortages.
Columbus Regional Healthcare System emergency department manager Donna Hill (left) listens as Sen. David Curtis (R-Denver) asks questions about the facility’s telehealth services. Photo credit: Rose Hoban
Veneziano, who relocated last year from New York City, said she never had an appreciation of what these types of services could mean to a rural community.
It costs $12,000 per month just for the telepsychiatry service, Veneziano said. Despite paying for the telestroke and telepsychiatry services to be present in their facilities, she said the hospital can’t bill for them, in part because the services use physicians who are in other states to deliver the consultations.
But Scotland Health Care System CEO Greg Wood said the hospitals can come out ahead, despite the cost. Wood told of how one of his former board members was on the receiving end of telestroke services during the previous week.
“This little R2D2 camera wheeled right in!” Wood said his board member told him. The man thought he was having a stroke. Within two minutes in the ER, he had a neurologist on the line to confirm that he did not need a stroke-busting drug.
The physician on the telestroke service was also able to determine the patient didn’t need to go to a larger medical center to see a neurologist, so he was able to have tests and recuperate in a hospital close to home for several days.
“It worked out well for the patient,” Wood said. “We’d never be able to recruit that capacity to a small town.”
Recruitment strategy: Attract residents
Wood and the others said that problems with recruiting medical talent was ongoing, describing difficulties finding doctors, nurses and other professionals for their facilities.
“We currently need 19 primary care physicians and 11 specialty providers,” said Southeastern Regional Medical Center CEO Joann Anderson. “We have had two OB physicians leave our community; a third is in the process of leaving. That leaves me with one full-time OB/GYN and one GYN.”
Each year, 1,500 babies are delivered at her facility.
“If you Google Robeson County, the statistics that come up are negative statistics, in terms of where you might want to live,” she said.
Anderson’s facility has partnered with Campbell University to provide a place for osteopathic physicians from the new medical school to perform post-academic training. But that comes with a big price tag.
“It was a little over $11 million for this year,” Anderson said. “The cost of that was the salaries for each of the residents, faculty costs, the location, the space that we had to provide for them, all the equipment they had to have. For example, we had to buy three ultrasound machines for them to use, each costs thousands of dollars.”
“A lot of things went into that figure.”
Anderson said she’s only starting to see the return on investment, four of the nine primary care residents completing training will stay there.
Columbus Regional Healthcare System emergency department manager Donna Hill (left) shows committee co-chair Rep. David Lewis around their facility. Photo credit: Rose Hoban
“We have four who have signed to stay in Lumberton, a fifth is in negotiations with me today, two … will stay in North Carolina in the western part of the state,” she said. “That’s just the beginning.”
She also said the hospital had more than 600 applicants for six slots for emergency medical residents.
On top of costs for residents, Anderson said her hospital spent about $8 million on contract nurses last year because of a local shortage.
Wood also spent millions on contract nurses and reiterated the need to train nurses at the local community college to keep them. He also pointed to the increasing trend of hospitals having to hire their physicians. To keep their long-time ear, nose and throat specialist, Wood had to pay dearly.
“He’s been pushing us for three years to help him run his practice, he keeps losing money,” Wood said. “He finally showed up and said I have two offers to leave town. He’s the only ENT in town. Do you want to employ me or do you want to see your ENT service lose?”
To employ him, Wood had to fix up his office, replace his computer system, hire more staff and pay him more.
“I had to go to the board and say, ‘We want to employ this ENT physician, something we used to get for free for his services and it’ll cost us a few hundred thousand dollars,’” he said.
His board approved.
Tip of the iceberg
The CEOs also discussed the skyrocketing costs for behavioral health patients that are currently filling emergency department beds, competition in their urgent care business, and high rates of uninsured, Medicare and Medicaid patients, who bring with them poor reimbursement.
Add to these challenges the federal budget has made cuts to programs to provide loan repayment for providers willing to serve in high poverty rural areas.
After tours of the emergency department and the cancer treatment center, Lewis said he was looking to roll out some relief in the upcoming legislative short session, that begins in May. He mused that the relief might take the form of changes to residency training reimbursement and paying for telehealth services.
“We said, if we can make one thing better, if we can make one person just a little bit healthier, then this will have been well spent,” Lewis said.
Looking for new locations where hunger hits the hardest, planners at Loaves & Fishes, a Charlotte-Mecklenburg County emergency food provider, used a sophisticated, layered mapping process born at UNC-Chapel Hill to find the right spots.
“Access to medical services is crucial to being healthy, but research shows that more than 70 percent of a person’s overall health is driven by social and environmental factors outside the health care system,” Dr. Betsey Tilson, state health director and DHHS chief medical officer, said in a statement.
The layered state guide, called a “story map,” lets users track information from 10 county-based public health regions across the state. The data show the chief non-medical factors — residents’ economic status, social and neighborhood conditions, and housing and transportation access — that can have overriding effects on community health.
Lighting up
“We wanted to make sure that the pantries we operate and those we open are in the right location,” said Tina Postel, executive director of Loaves & Fishes in Charlotte. “One of our pantries that we opened was at Hope Covenant House. It’s in an area that we didn’t have a pantry, but it lit up bright green on the map.”
A look at the DHHS map shows that Region 4, Tract 45 of Mecklenburg County, where the community-development corporation Hope Covenant House is located, is home to 3,146 people. Almost three out of four have poor access to grocery stores, making it a natural market for a new food pantry, Loaves & Fishes decided in 2016, based on data from a pilot map.
Screen shot of the social determinants map showing poor food access in a region of northwest Charlotte.
“We’re taking these findings and data to a larger group of stakeholders to design interventions,” said John Wallace, a data analyst with the Institute for Public Health. “It’s not necessarily guiding the intervention.”
Low access to food was defined for the study as living more than a half mile from a large grocery store in an urban setting, or in a rural setting living more than 10 miles from a large grocery or supercenter.
In contrast to Tract 45 north of downtown Charlotte, everyone of the 2,285 people in Mecklenburg’s Region 4, Tract 58.29, had adequate access to grocery stores, according to state and federal statistics used by the mapmakers. The tract is about 16 miles south of Hope Covenant House, almost in South Carolina.
This segment of Mecklenburg County has no issues with access to fresh, healthy food, as shown on the new maps.
Another key number shown by the map is what’s called the z-score, the amount by which the combined social determinants in a given area, in this case a census tract, vary from the average in the region of counties. The z-score for the area where Loaves & Fishes placed the new pantry shows that the tract was among the region’s greatest deficiencies in the areas considered.
Locating and fixing such problem areas is the heart of the mapping effort, state officials said.
“No matter what our respective goals — to mitigate the opioid crisis, to ensure our children are healthy, safe and ready to learn, to increase employment or to drive economic growth — it all begins with healthy people,” Dr. Mandy Cohen, DHHS secretary, said in a statement.
Regional comparisons
A measure called the Social Determinants of Health Index combines indicators into three groups, each with equal weight in determining a final score. The individual and overall scores are compared to other counties in the same region, making statewide comparisons unrealistic.
“If you’re a coastal tract in Brunswick, you’re comparing yourself to every county in the state and it loses a lot of its usefulness,” said Matt Simon, a GIS analyst at the public health institute. “It makes more sense to compare it on a region-by-region basis.”
Still, it’s inevitable that users will find their own ways to use the map’s wealth of information, not all of it medical. Want to know the median income in Wake County? It’s $70,620, compared to $31,129 in Bertie County in Northeastern North Carolina.
Interested in the rate of people living below poverty levels in the west side of Lumberton, where Hurricane Matthew ripped up homes, churches and businesses? It’s 54.1 percent, compared to 10.6 percent living below poverty in a tract just west of booming Asheville.
Numbers such as these can suggest projects in the making for public, private and nonprofit interests.
“I think that that’s one way that the tool could be used, to figure out where resources are lacking,” Wallace said. “This is basically a conversation starter.”
The map has roots in a pilot project in which the public health institute combined forces with the Carolinas HealthCare System (now known as Atrium Health) to map a 10-county region including CMC’s own Charlotte campus. Another iteration of it is taking place in Raleigh under the auspices of the John Rex Endowment.
So far, there are no plans or funding to make the state map part of a longitudinal effort, such as the one seen the annual county assessments by the Robert Wood Johnson Foundation.
“We would love to say yes to that,” Wallace said. “We really want to do this long-term.”
Will Cain drove the carcass of a dead calf from Cumberland County to a state lab in Raleigh early this month hoping someone, someday can tell him if chemical pollution harmed it.
Cain raises beef cattle on multiple plots north of the sprawling Chemours chemical factory property south of Fayetteville, including land about two miles away. Like some farmers nearby, he wonders if recently detected chemical pollution from the plant in air, soil or water threatens his livestock or other food raised nearby.
“The consumer has the right to know,” said Cain, who sells cattle to feedlots in corn-rich states such as Kansas to fatten them up before they are slaughtered and their meat readied for market.
Let’s be clear: Aside from a GenX chemical found in one sample of local honey, there is no publicly known evidence that industrial pollution released by Chemours or DuPont, the previous owner, has tainted foods raised nearby.
State officials are still assessing whether testing is needed in the vicinity of company’s 2,150 acres. Developing a means to conduct meaningful tests of food, they stress, would be a complex task that will take time.
For one, they would need to find or develop methods that detect per- or polyfluroalkyl (PFAS) compounds such as what is commonly called GenX in very different types of organisms, potentially from blueberries to swine. State officials also would need solid data on levels at which contamination could pose a risk to people or the environment.
“You can’t just collect samples of a turnip crop or a collard crop in someone’s garden, send it to the lab, get back a range of values, and not be able to tell the public what it means. We want to be able to say whether it’s safe in food or soil or groundwater,” said Michael Scott, Division of Waste Management director for the state Department of Environmental Quality.
Big challenge
Scientists around the world are raising alarms about PFAS chemical contamination because it potentially carries a triple threat. The chemicals are so tough that they don’t break down in nature; they can accumulate in the tissues of people and other living things, including edible plants; and some bring known or suspect health risks.
Because the compounds are soluble in water, they don’t stay in one place either, instead traveling down rivers, through soils and with rain storms.
PFAS chemicals originating from the Chemours site, on the border of Bladen and Cumberland counties, have been found in residential drinking wells three miles away, in rainwater collected at seven miles distance, and many tens of miles away in drinking water drawn from the Cape Fear in and near Wilmington.
A portion of the industrial compound that Chemours operates on some 2,000 acres wedged between the Cape Fear Riiver and NC Route 87, right where Cumberland and Bladen counties meet. Photo credit: Catherine Clabby
So do plants or animals living close by harbor the chemicals too?
“The food is the next frontier,” said N.C. State University scientist Detlef Knappe, one of the small group of researchers who first detected Chemours chemicals in drinking water in this state.
Members of his laboratory have collected some food grown near Chemours but high-confidence testing remains a work in progress, Knappe said.
Signals from afar
Signals exist that food could be a concern.
In Ohio and West Virginia communities exposed to PFAS released by the DuPont plant now owned by Chemours, people who ate locally-grown vegetables had higher blood levels than others who didn’t. (Blood and urine of North Carolinians downstream of Chemours have been collected too but results are not yet known.)
Sampling has detected PFAS compounds in home gardens near PFAS pollution sites abroad and in Minnesota. Small amounts of GenX were found in plants grown very close to a Chemours plant in The Netherlands, for instance.
Researchers at both locations concluded that the detected amounts in the two spots were low enough that people did not need to stop eating food from their gardens in both places.
But you can’t use studies made at one polluted place to determine risks from PFAS contamination in another place, said Deanna Scher, the principal epidemiologist, and James Kelly, a surveillance and assessment manager at Minnesota’s Department of Health.
That’s because contamination levels and other factors differ, just one part of the difficulty of assessing risks from unregulated PFAS that did not undergo rigorous, publicly disclosed health testing before being put to work, they said. “It’s frustrating to have to learn after the fact when the horse is out of the barn and to explain to people we don’t have many of the answers,” Kelly said.
State health officials in North Carolina are testing fish caught in polluted waters near Chemours for PFAS. If comprehensive agricultural testing happens here, it appears that the job will be split between state environmental and agriculture departments.
A memo written by Joe Reardon, assistant commissioner for the N.C. Department of Agriculture and Consumer Services, recommended that DEQ officials focus any sampling they conduct “on commodities that are not entering commerce.”
That’s because the agriculture agency has jurisdiction over marketed agriculture, Reardon said.
Plus, testing without solid information about the risks from contaminants could give inaccurate impressions, said Reardon and agriculture department public affairs director Andrea Ashby.
“We are concerned that the collection of samples without an approved method or toxicological standard to reflect the significance of the findings could create unnecessary consumer anxiety and could negatively affect products’ ability to move in commerce,” Ashby said
Scott, the DEQ director, and NCSU’s Knappe agree that reliable testing and risk assessments standards are needed. Toxicologists with DEQ and the state Department of Health and Human Services are exploring what’s known, Scott said.
State officials until now have depended on a state provisional health goal of 140 parts per trillion as the threshold above which consuming GenX chemicals in drinking water over a lifetime has been posited to pose a health threat.
The US Environmental Protection Agency this summer is expected to release its awaited toxicity assessments for two forms of GenX chemicals, the dimer salt version and another version of Hexafluoropropylene oxide (HFPO), compounds used in the industrial process that Chemours calls GenX.
EPA is also expected to quantify a reference dose, the amount of chemical someone can ingest for a lifetime without anticipating harm.
Waiting
Cain, who drove that calf carcass to the state Rollins Animal Disease Diagnostic Laboratory in Raleigh this month, grew concerned about possible contamination after five calves in his herd of about 200 died during a 10-day span this month, he said.
Cain had sold cows to a close friend, Jeremy Singletary, who lost five calves and adult cows on land about three miles north of Chemours he said he rented about two years ago.
Singletary said a friend froze one dead calf in case it could one day be tested for PFAS contamination.
“I’m not going to sit here and tell you GenX is killing my cows,” Singletary said by phone on Tuesday. “But I do need to know some type of answer.”
Low levels of GenX were recently detected in Robeson County, across the river from Chemours, in its water system and in a swamp about seven miles from the plant. It’s been detected in drinking wells there too.
William Canady, a fifth-generation farmer based in Robeson County, said he has not had mysterious problems with cattle, which he also raises about seven miles from Chemours. But he would like to know if any industrial compounds can be detected in his animals or among the long list of produce he raises for sale, including field corn, sweet corn, soybeans, oats, strawberries and watermelon.
“A lot of people work at that plant. I think the pay can be pretty good,” Canady said. “I just hate to see it doing damage to the community.”
To be cautious, he no longer feeds his cows any of the hay Chemours allowed him to harvest on its property the year before last.
He also wonders if the state has more options than testing commercial livestock to start getting a look at whether PFAS chemical may be tainting meat.
“There are a lot of deer right around that plant,” Canady said. ”They ought to test those deer. And move out from there.”
When it comes to your health, place matters. If you live in a rural county, the bottom-line truth is that you’re less apt to be healthy than if you lived in a more urban one. A couple of recent reports shed some light on both the issues and potential solutions.
According to the 2018 County Health Rankings, published by the Robert Wood Johnson Foundation in partnership with the University of Wisconsin Population Health Institute, rural counties continue to lag behind more urbanized ones in factors that play a critical role in a community’s overall health. These include child poverty, low-birthweight babies and teen birth rate.
But rural communities have within their DNA the resources to rise to these challenges.
In another report, titled “Exploring Strategies to Improve Health and Equity in Rural Communities,” researchers at the University of Chicago’s NORC Walsh Center write that while much of the research exploring rural health issues in the U.S. focuses on disparities – increased health risks “related to geographic, socioeconomic, environmental and other factors” – seldom is attention paid to the strengths and assets within these communities that can be, and often are, deployed to improve health.
These communities’ greatest assets, the researchers assert, are their people: “Commonly reported individual assets include civic and community engagement in the form of volunteerism, strong entrepreneurship, and the resilience and adaptive capacities of rural residents.”
The County Health Rankings report is a call to action. It petitions community “changemakers” to explore the data to better understand the nature of the challenges, and to then more fully leverage assets within the community to address them, implementing strategies that will allow every community member to lead the healthiest life possible.
To advance this initiative, the County Health Rankings & Roadmaps program sends coaches out to assist individual communities.
“We’ve been partnering with the National Association of Counties for the past two years on the Rural Impact County Challenge, working with counties who bring teams together to think about opportunities to take action addressing children in poverty,” says Aliana Havrilla, one of those coaches. “But in my experience, it’s become a much broader conversation about opportunities and assets that exist at the local level.”
Slow recovery
The County Health Rankings underscore the primary role poverty plays in health outcomes and indicate that while child-poverty rates are declining, they remain at levels higher than before the recession.
“In the wake of the Great Recession, rates of children in poverty stayed high through 2012 and, despite declines in recent years, remain higher than the pre-recession era,” says Anne Roubal, a population health analyst for the Rankings & Roadmaps program.
Rates of recovery, she stresses, vary by place and race. “In general, child-poverty rates have not bounced back in many rural counties or those with a greater share of people of color.”
Rural counties continue to have the highest child poverty rates (23.2 percent) followed by large urban metro (21.2 percent), smaller metro (20.5 percent) and suburban counties (14.5 percent).
The County Health Rankings authors write that poverty limits opportunities and increases the likelihood of poor health. Children living in poverty are less likely to have access to quality schools and have fewer chances to prepare for living-wage jobs leading to upward economic mobility and good health.
“Children in poverty is an upstream measure that assesses both current and future health risk,” they write. “Recent data on poverty show that rates among children and youth are at least 1.5 times higher than rates among adults aged 18 and older.”
Disparity among neighbors
Health outcomes in the County Health Rankings are measured by how long people live and how healthy they feel. Length of life is measured by premature death – deaths that occur before individuals reach their statistical life expectancy. Quality of life is measured by the percentage of days people report poor or fair health, the percentage who report physically and mentally unhealthy days within the past 30 days and the percentage of low-birth-weight babies.
The disparity between rural and urban counties in these measures and others is often stark.
Take, for example, the North Carolina counties of Wake and Robeson. Wake County, where Raleigh, the state capital, is located, is part of a thriving metropolitan area with more than 2 million residents. It ranks first in the state in the report’s health outcomes.
Robeson County, an hour-and-a-half drive to the southeast, is largely rural. The largest city, Lumberton, has a population of about 21,000. It’s ethnically diverse, roughly 40 percent Native American, 30 percent white and 25 percent black. Robeson ranks last, 100th, in health outcomes in the state.
Data, visualization courtesy: NC Child
County Health Rankings data indicate that Robeson County residents reported more than twice as many days being in poor or fair health than Wake County residents (29 percent vs. 13 percent). Nearly twice as many Robeson County residents reported physically unhealthy days within the past 30 days (5.4 percent vs. 2.9 percent) and more reported mentally unhealthy days (5.4 percent vs. 3.6 percent). A Robeson County adult is also much more likely to be obese (39 percent vs. 23 percent).
The data further indicate that there are more than two and a half times as many premature deaths each year in Robeson County than in Wake County.
Now consider poverty. Its correlation with poor health outcomes is underscored in the contrast between these two counties.
Robeson County has the highest rate of poverty in the state, among the highest in the country. Nearly a third of all residents live below the federal poverty level (in 2017, $24,600 for a family of four); nearly half of all children live in poverty. Almost twice as many Robeson residents as Wake residents are unemployed (7.9 percent vs. 4.2 percent) and twice as many are uninsured (20 percent vs. 10 percent).
Lumberton, the county seat of Robeson County, is 100 miles and a world of difference from Raleigh.
Local connections
“Things are improving,” Anne Roubal says of the national outlook – slowly. “Starting in 2008, we saw a jump in poverty pretty much everywhere and that trend continued for three years.” Things then began to improve, but not as quickly as they’d gone into decline. “We’re still not back to where we were in 2006 and 2007.”
The resources needed to recover and to build healthier communities are found in rural America. Health care institutions in many rural regions are taking innovative approaches to meeting their communities’ needs. In Robeson County, the local hospital, Southeastern Health, is tackling its community’s health care issues by remaining independent and offering a broad range of care under one roof.
But it’s often individuals who step forward. According to the NORC Walsh Center report, “participation in community life in rural areas often stems from strong individual relationships and connections that people form with one another.” Such connections “lead people to participate in volunteering, community organizing and coalition building.
“One thing I really appreciate about rural communities is that they have a culture of such strong collaboration,” Aliana Havrilla says. “Sometimes, it’s everybody knows everybody because many people wear many hats. There’s also often just that tight-knit community feel … a strong asset-based collaborative approach that they’re bringing to this work addressing complex issues.”
When it comes to health care, one of the biggest problems faced by rural residents often is finding a doctor, dentists or other practitioner near home.
A bill unveiled in the waning days of the annual legislative work session seeks to find ways to incentivize more medical providers to settle – and stay – in rural North Carolina.
“If individuals practice, or learn or are educated in rural areas, they tend to stay in rural areas,” Rep. Greg Murphy (R-Greenville) told his fellow lawmakers this week as he moved a bill that will study what it takes to get and keep health care providers in rural burgs.
Lawmakers spent last winter on two different committees which were dedicated to examining health care workforce issues throughout North Carolina. One of those committees sought ideas on the best ways to improve health care access in rural parts of the state, the other, headed by Murphy, looked at how to help induce physicians to practice in rural areas.
One way to do that is to create more training opportunities in rural areas themselves. To that end, the bill orders the Department of Health and Human Services to identify which rural hospitals could become teaching facilities and figure out what they’d need to become successful.
“Take Ahoskie, for example, it is a very rural hospital, has a 120 bed system,” said Murphy. “It’s putting family practitioners, family practice residents to rotate out in those areas, it’s possible to put internal medicine residents there … just a rotational thing.”
But making the conversion to instruction is no easy task, said Southeastern Health CEO Joann Anderson. Her Lumberton-based hospital partnered with Campbell University to start a medical residency program which will graduate its first students this month. Four of the primary care residents signed up to stay in Lumberton, another two will move to rural Western North Carolina. The program has also recruited education slots for family doctors and emergency medicine.
Sponsored
“This year, we had six slots for emergency medicine, we had more than 600 applicants,” she told lawmakers this March when the rural health care access committee visited Columbus County.
But to do this is expensive. Anderson described the dollars spent on startup costs, enhanced salaries to attract faculty and students, and equipment.
“It was a little over $11 million for this year,” Anderson said. “The cost of that was the salaries for each of the residents, faculty costs, the location, the space that we had to provide for them, all the equipment they had to have. For example, we had to buy three ultrasound machines for them to use. Each costs thousands of dollars.”
The bill also instructs DHHS to rejigger its North Carolina State Loan Repayment Program to help people practicing in rural areas shed their debt, with an eye toward recruiting new providers to small towns and getting them to stay there.
Dentist credentialing gets nod
And, at the last minute, lawmakers inserted a provision to make it easier for dentists from the neighboring states of Virginia, Tennessee, Georgia and South Carolina to become licensed in North Carolina.
In the past, dentists from other states have had to jump through multiple hoops to obtain a license to practice here. Until now, North Carolina has only accepted dentists who have passed a credentialing exam that’s accepted in only seven other places: Alabama, Louisiana, Puerto Rico, the US Virgin Islands, West Virginia, Arkansas and Utah. Dentists from states other than those have had to submit to a recredentialing process that can take months and cost thousands of dollars.
In some quarters, this has been seen as a block to getting more dentists into North Carolina, which has historically had fewer dentists per capita than most other states. Three counties in the state have no dentist and the state consistently ranks 47th among the 50 states in terms of dentist-to-population ratio.
Map caption: North Carolina has about 4.7 dentists for every 10,000 people. Nationally, the ratio is closer to about 6.2 dentists for every 10,000 people.
“That certainly may have an impact on addressing the dental workforce capacity in counties adjoining the neighbor states, particularly in our more rural counties,” wrote Lewis Lampiris, who trains students in community dentistry at UNC-Chapel Hill’s dental school.
Lampiris noted another important change, namely loosening restrictions on dentists who receive these licenses “by credential.” Currently, dentists licensed by credential have to choose only North Carolina as a location for practice; this has limited the ability for dentists in towns along North Carolina borders to open up a satellite office across state lines.
The bill removes that restriction.
The Senate passed the bill with little debate. But Sen. Erica Smith (D-Jackson) said the bill falls short in one important way.
“The elephant in the room and in this bill is the lack of opportunity to study Medicaid expansion,” Smith said.
“How do you improve rural health care?” she asked. “You expand [Medicaid].”
Historically, the residents of rural Robeson County have relied heavily on the Southeastern Health Emergency Department for much of their medical care, even for non-emergent issues such as sore throats and sprains.
The hospital, located in the county seat of Lumberton, has about 90,000 ED visits per year, according to Southeastern Health CEO Joann Anderson.
The front desk of Southeastern Health’s Walmart urgent care. It’s is a three-room clinic that serves as a place where patients can get their non-emergency health needs taken care of quickly without going to the hospital’s Emergency Department. Prices are clearly listed on the wall at the entrance. Photo credit: Taylor Knopf
“If you ask a lot of people in Robeson County who their primary care provider is, they are going to give you an emergency department physician name,” Anderson told the legislative Committee on Access to Healthcare in Rural North Carolina earlier this year when lawmakers traveled to Columbus County to meet with hospital CEOs and rural health providers.
ED overuse is not just a problem in Robeson County. The hospital CEOs from Columbus and Scotland Counties also told state lawmakers about similar issues in their communities. All these health care CEOs want patients to instead use urgent care clinics for non-emergency conditions such as the flu, a urinary tract infection or minor cuts.
“There’s really no reason for them to be there,” Anderson said. “So how do we make that happen?”
A price list for common procedures and visits to the Walmart/ Southeastern Health clinic, complete with ICD-10 codes. Photo credit: Taylor Knopf
The answer has come with making urgent care clinics easier to get to than the hospital. In Lumberton, that means there’s an urgent care right inside the entrance of the local Walmart.
Overused
All the CEOs said there’s several reasons why it’s hard to break the habit of turning to the emergency room for everything. For starters, there are uninsured people who use emergency departments because they know they can’t be turned away. That’s because once a patient sets foot inside an emergency room, providers there are obligated by federal law and other rules to treat and stabilize them.
In Robeson County, Anderson said she doesn’t know exactly how much money her ED loses each year, but said Southeastern Health’s finances have little room for error.
“The operating margin for the last five years has been about 1.3 percent, which is low,” she said. “Last year we actually lost money.”
Southeastern Health looks to its walk-in urgent care clinics – including the Walmart location – to take the pressure of the ED. Anderson said the Walmart site is “unique” and is one of Southeastern Health’s busiest.
Prices are posted on the wall, so patients know exactly how much they are going to spend. And since it’s located inside a major shopping destination, many customers see it. Plus, Walmart’s pharmacy is located nearby, so patients can get their prescriptions filled immediately.
Inside Walmart
Will Von Taborsky works at the Walmart vision center just next to Southeastern Health’s urgent care clinic. He finds the clinic to be very helpful for his family and his boy scout troop.
Will Von Taborsky is the Walmart vision center manager which is located right next to Southeastern Health’s urgent care clinic. He said his family will frequently use the clinic for colds and other non-emergency health needs. He said it’s also a great place to get a quick sports physical for a decent rate. Photo credit: Taylor Knopf
“We’ve used it as a family for personal things like colds and flus and shots and that type of thing,” he said. “But the other thing I find it very convenient for, hanging out with young people in the community, is sports physicals or summer camp physicals.”
He’s the scout master and will tell parents the walk-in clinic is a “quick, easy and inexpensive” place to get that last-minute physical. Those are only $25.
If you don’t have health insurance, a sick visit at the Walmart clinic is $65.
Brooke Grooms is a nurse practitioner there. She said compared to other urgent cares, the Walmart location is a “fast-paced, ‘street and treat’ kind of clinic.”
It only has one exam room.
“They are in and out within 15 minutes,” she said. “We don’t see complex issues here, just sinus infections, colds, flu… There are times where I’ll do more complex things like suturing, abscess drainage, but that’s only if I don’t have a line.”
She sends those needing more advanced care to the Southeastern Health’s “mall clinic,” which has four patient exam rooms, more staff, and the ability to set fractures and perform X-rays.
Southeastern Health’s Walmart urgent care is a three-room clinic that serves as a place where patients can get their non-emergency health needs taken care of quickly without going to the hospital’s Emergency Department. Photo credit: Taylor Knopf
“If we see it’s something where there’s chest pain, shortness of breath, and high blood pressure, they go straight to the ER,” Grooms said. “If they look bad enough, we can call the ambulance.”
She said she’ll see some of the same patients over and over.
“Some are regular Walmart shoppers,” she said. “We are the only Walmart with a clinic. People walk by and see us.”
Grooms emphasized that she is not a primary care provider, even though many patients try to treat her as such. She can give prescriptions refills on a limited basis, because she said it can be difficult to get in to see a primary care provider.
Her mother was a primary care doctor in Robeson County for 27 years, and Grooms said her mom frequently saw her patients the same day they called. But that’s not the case anymore.
Sponsored
Grooms said she believed the urgent care clinics take the load off primary care offices more than the Emergency Department.
“I use to be an ER nurse. It was bad. We had 13-15 hour waits, and a lot of this county is unemployed,” she said. “With unemployment comes no insurance. The only place in town that will see you regardless of anything is the ER.”
Across from the hospital
Another way Southeastern has sought to divert patients on their way to the emergency room is by placing another urgent care clinic right across the street from Southeastern Health’s hospital emergency department.
The “health mall” across the street from the Southeast Health’s main hospital is a place where hospital leaders are encouraging patients with less emergent problems to get seen. Photo credit: Taylor Knopf
Barry Graham is a physician assistant there in the “health mall.” He said it’s difficult to say how many patients come to the urgent care instead of the ED. Some people definitely walk into his clinic who should be getting emergency care.
The health mall is in a strip mall next to a JC Penny and has a variety of providers and services. Within the health mall, there is an express lab, an urgent care, a pharmacy, a surgical center, weight loss center, and a diabetes community center.
The health mall urgent care clinic is open Monday through Friday from 8 a.m. to 5 p.m., as well as some weekend hours and Graham said the clinic is in the process of expanding to evening hours. He sees about 30 patients a day, which is more than most primary care providers will see in the same time period.
But Graham agreed with Grooms, saying his clinic likely takes more pressure off of primary care physicians with busy offices than the ED.
“I mean, they try to see walk-ins but, but you know, especially as it gets later on in the day, it’s hard to have a walk-in,” he said. “They feel comfortable having folks come see us.”
As floodwaters from Hurricane Florence continue to rise in some areas, clean water advocates, state regulators and national attention are turning to the nasty mix of pollutants heading downriver and downstream here.
As reported Friday, floodwaters from the Cape Fear River breached Duke Energy’s L.V. Sutton facility in Wilmington. Water flowed into Sutton Lake on the north side and back into the river on the south side.
The N.C. Department of Environmental Quality said a thorough investigation of events would soon follow and that Duke Energy would be held responsible for any environmental damage. An EPA coordinator and NCDEQ staff met with Duke Energy and personnel at the Sutton facility Monday to survey conditions, according to a tweet late Monday by EPA Southeast.
Overview of Duke Energy’s LV Sutton plant in Wilmington shown from the northwest on Sept. 22. Photo credit: NC DEQ
DEQ said Sunday that 32 waste lagoons at 27 swine operations were discharging into floodwaters. Lagoons at five facilities showed structural damage, although DEQ said that means the lagoon may or may not be discharging. Another seven facilities with nine lagoons were inundated, with water surrounding and flowing into the lagoons and 16 facilities with 18 lagoons were full and likely to spill over. As many as 31 facilities, or 39 lagoons, were 3 inches or less from being full.
In some flood-prone area beach towns, officials were allowing the pumping of stormwater in nearby ponds, sounds and the ocean.
Bogue Banks beach towns were this week using pumps to address the flooding in neighborhoods, where streets have been impassable and septic systems failing. Towns including Pine Knoll Shores and Emerald Isle were still pumping Monday and advising the public to avoid contact with standing water.
Officials in Pine Knoll Shores noted Saturday that the town had been pumping into golf course ponds, the man-made canal that loops through town and into the ocean, as permitted during emergencies.
In Emerald Isle, pumping in some areas alleviated the flooding, but groundwater seeped in and caused these areas to flood again. The town said pumping would continue until water levels stabilize.
Larry Baldwin, the Crystal Coast Waterkeeper based in Morehead City, said he was investigating water quality issues on Bogue Banks Monday. He noted several locations where stormwater was being pumped out of neighborhoods and into the ocean or sound, but one location was especially foul.
“This particular one smells absolutely horrible,” Baldwin said of the water being pumped to the ocean from the Land’s End development off Coast Guard Road in Emerald Isle. “This water coming out of Land’s End is different from the stormwater we see coming elsewhere in Emerald Isle.”
Sponsored
Baldwin said he’d seen people during the weekend walking through the drainage.
“I’ve got a lot of concerns,” he said. “Everybody here is on septic. We’re doing basic bacterial testing and taking samples to a lab in New Bern. I understand communities don’t want to flood but what are we doing environmentally just pumping this stuff where ever we want it to go? Somebody’s got to be looking at this water just from a public health standpoint.”
State recreational water quality officials before the storm gave notice advising the public to avoid swimming in all coastal waters of North Carolina following Hurricane Florence.
“Excessive rains and flooding can cause high levels of bacteria in the water that can make people sick,” J.D. Potts, manager of the N.C. Recreational Water Quality Program, said in a statement. “Floodwaters and stormwater runoff can contain pollutants such as waste from septic systems, sewer line breaks, wildlife, petroleum products and other chemicals.”
This pair of NASA satellite images shows how the flood has affected water quality in the White Oak River, New River, Adams Creek, and their outflows along the coast on September 20, 2018. The natural color image from Landsat 8 reveals how soils, sediments, decaying leaves, pollution, and other debris have discolored the water in the swollen rivers, bays, estuaries, and the nearshore ocean. The second image combines visible and infrared data from Landsat to reveal the amount of colored dissolved organic matter in those waterways. Organic matter—such as leaves, roots, or bark—contain pigments and chemicals (such as tannins) that can color the water when they dissolve. Depending on the amount of dissolved particles, the water in natural-color imagery can appear blue, green, yellow, or brown as the colored dissolved organic matter concentration increases. Photo credit: NASA
The notice listed as hazards the pumping of floodwaters, sanitary sewer malfunctions, overflowing manholes and lift stations failures which could discharge into coastal waters.
Shellfish Sanitation and Recreational Water Quality officials issued Monday precautionary advisories for a large portion of the coast and updated its recreational mapping site.
Under the state Department of Environmental Quality, DMF Headquarters in Morehead City closed on Sept. 11 and Section Chief Shannon Jenkins expects it to open Thursday. The lab was temporarily unavailable because of HVAC issues, which Jenkins said affects a step in the testing process.
The DMF Central District Office in Morehead City also closed Sept. 11 and reopened Monday. “We did work out of the office during this time period as available to document and assess sewer overflows/flooding etc. and provide situation reports to the department,” Jenkins said in an email.
The division’s Wilmington Regional Office was closed Sept. 13 and will not reopen before Sept. 28 because of damage and safety issues.
Jenkins said that regarding shellfish, except for northern waters that didn’t experience the same rainfall or storm impacts, they don’t anticipate sampling the shellfish growing waters this week. “With the rainfall amounts alone, we wouldn’t expect the central/southern waters to return to normal anytime soon with the lands still draining.”
They will continue to assess wastewater overflows and flooded areas with Department of Water Resources and municipalities, which would have an impact on sampling plans, he added. “We will have more information as this week progresses.”
Damage Estimates
Although several rivers were above flood stage and seven river systems at major flood stage Monday, there were signs that recovery is in full swing in southeastern North Carolina. The full extent of the damage, however, is just starting to become clear.
Damage estimates from Hurricane Florence are rising and in a mid-afternoon update, Gov. Roy Cooper put to rest any comparison that ranks 2016’s Hurricane Matthew higher in terms of total devastation.
Gov. Roy Cooper speaks during the 5 pm briefing on Thursday, Sept. 13. Screenshot of video UNC TV video feed.
Cooper said the number of people applying for Federal Emergency Management Agency assistance so far is already close to the total number of applicants who applied after Matthew. The state has recorded 35 storm related deaths so far.
“We’re going to see significantly more people affected by this storm and it is much more widespread than Matthew,” Cooper said.
Many areas were hit hard in both storms, he said, a fact that the state will have to reckon with as it considers how and where to rebuild.
FEMA Disaster Recovery Centers opened in Onslow, Carteret and Pamlico counties to assist those affected by Hurricane Florence. The centers offer in-person support from FEMA recovery specialists, the U.S. Small Business Administration, the state and others.
The center in Jacksonville is next to Don Williamson Nissan at 312 Western Blvd. Hours are 9 a.m. to 7 p.m. Monday through Saturday and 9 a.m. to 1 p.m. Sunday.
The Disaster Recovery Center in Morehead City is at the Carteret County Health Department, 3820 Bridges St., Suite A. Hours are 9 a.m. to 7 p.m. until further notice.
The FEMA Disaster Recovery Center in Pamlico County is in Grantsboro Town Hall, 10628 NC Hwy. 55 East, Grantsboro. Hours are 9 a.m. to 7 p.m. Monday through Saturday and 9 a.m. to 1 p.m. Sunday.
Applicants must register online at www.fema.gov or by phone at 800-621-3362 prior to visiting the center to complete the application process.
North Carolina homeowners, renters and business owners in Beaufort, Bladen, Brunswick, Carteret, Columbus, Craven, Cumberland, Duplin, Harnett, Lenoir, Jones, New Hanover, Onslow, Pamlico, Pender, Robeson, Sampson, and Wayne counties may apply for disaster assistance for uninsured and underinsured damage and losses resulting from Hurricane Florence.
Moody’s Analytics has estimated the economic damage from Florence could be as much as $50 billion, the Wall Street Journal reported. Available local estimates are just a starting point.
Initial damage assessments were completed Friday in New Bern. Final numbers according to the city’s website are $74.5 million in residential damage from Hurricane Florence and $25.6 million in commercial damage.
Across Craven County, about 1,100 structures sustained major damage and 2,600 structures had been reviewed.
“As of right now, Craven County has $87.5 million of assessed damage and that figure is counting,” said Amber Parker, the county’s human resources director. “The damage assessments are ongoing as Craven County has a very large area to cover.”
Cornelius J. Jordan, Onslow County’s communications director, said Monday that county is still in the process of damage assessment. Jordan followed up Tuesday with preliminary numbers.
A barn destroyed during Hurricane Florence by a suspected tornado in Carteret County, near Newport. Photo credit: Rose Hoban
Total count for damaged residential structures, ranging from minor damage to destroyed, in unincorporated areas of Onslow as of Monday morning was counted at 7,212, at a total of $245,492,848. For businesses in unincorporated areas, the total came to 154 and at an estimated loss of $24,662,858, as of Tuesday morning. Jordan reiterated that the damage assessment is ongoing.
Onslow County Manager David Cotton informed the board of commissioners Friday during a special meeting that CrowderGulf, the debris removal contractor, has estimated that from the storm, the inert debris, such as leaves, limbs and logs, is 200 to 300 cubic yards and the construction and demolition debris — bricks, shingles, wood, sheetrock — is 100,000 to 200,000 cubic yards.
Jordan told Coastal Review Online that although flooding was a concern, the most widespread damage was from leaking roofs.
Around the county as a whole, Jordan said that the number of blue tarps covering roofs shows that rain getting inside homes and causing interior damage is a huge concern.
He encourages county residents to report damage using the survey report on the county’s Hurricane Florence website to let the assessment team know where there is major damage.
“Though it may not look it from the front, there may be major damage on the inside (of a building),” he added.
In North Topsail Beach, Mayor Dan Tuman reported that about 874 structures had sustained minor damage and an estimated 77 structures had major damage. A team from the North Carolina State Building Code Enforcement Office arrived in town Wednesday to help identify properties “not fit for habitation and might be at further risk should they be connected to the town’s present water and electrical service,” according to an email Tuman sent to town residents Wednesday.
The governor said that with more rain coming residents should remain cautious.
“Even as recovery starts, serious risks remain in Southeastern North Carolina,” he said. Flooded roads are still making travel dangerous and many communities are still on boiled water alerts.
Special Session Set
The governor’s office also announced late Monday that a special legislative session will start Oct. 2. Cooper had first set the date a week later, but legislative leaders said they plan to get started on disaster-related policy matters before adjourning until Oct. 9 to allow time for the Cooper administration to put together its recovery funding request, WRAL.com reported. In addition to funding, school systems in hard-hit areas are expected to receive a waiver on calendar requirements.
The governor said his main concern over the timing of a session was to make sure it was safe to travel to and from Raleigh for anyone who wanted to attend the session.
Shortly before the governor’s Monday afternoon briefing, state Department of Transportation engineers cleared Interstate 40 for travel to Wilmington, reopening the main land route to the city after flooding shut it down more than a week ago.
Truck traffic to the state ports in Wilmington and Morehead City also resumed service Monday and on Sunday night, the DOT reopened Interstate 95 and U.S. 74. DOT Secretary Jim Trogdon said on Monday that waters covering the roads receded quicker than expected and crews determined there was no significant structural damage.
That wasn’t the case for one key route into New Hanover and Brunswick counties. Trogdon said damage to the roadway of U.S. 421 at the New Hanover-Pender county line will require major repairs. In all, about 400 roads, most of them in eastern North Carolina, remain closed.
The damage caused by Florence to I-40 at mile marker 420 in Wilmington. Photo credit: NC Department of Transportation
Concerns about a potential break in a water line that runs under U.S. 421 were alleviated after emergency repairs over the weekend. Crews from the Cape Fear Public Utility Authority worked from the Lower Cape Fear Water and Sewer Authority’s raw water main that runs roughly 20 miles from the Cape Fear intake near Lock and Dam No. 1 to the city’s treatment plant.
The line runs underground in the area where the highway was damaged. In a statement released Monday, CFPUA officials said they would continue to monitor the water line to avoid any disruption of service. After Hurricane Matthew, a failure in a main due to flooding near Riegelwood required weeks of mandatory water restrictions.
Interstate 95 opened to traffic over the weekend after portions of the major artery were closed since Sept. 15. As of Monday, 415 road closures remained statewide. According to the NCDOT website, US-74 was open from I-95 to Wilmington and U.S. 70 was open between I-95 and the coast with one lane closed in each direction in Kinston.
Motorists should avoid unnecessary travel in Brunswick, Columbus, Duplin, Pender, Robeson, Sampson and Scotland counties due to the flooding or washout of multiple North Carolina and secondary routes. The department also recommends avoiding Bladen and Wayne due to the flooding and washout of multiple major travel routes.
Across southeastern North Carolina, seven rivers were at major flood stage Monday and three were at moderate flood stage. Additional rain was forecast for Tuesday and Wednesday in some areas.
Well Testing
Cooper urged those who use private wells to get them tested at their county health department before assuming the water is safe to drink.
Free water sampling kits for New Hanover County residents with private water wells are available from the county public health department. Officials in a notice recommend testing wells flooded as a result of Hurricane Florence to ensure there is no contamination. Ingesting or being exposed to contaminated well water may cause sickness.
Newport resident Glenn Skinner flushes his well, which was submerged in the floodwaters of Hurricane Florence as the storm pushed ashore. Photo credit: Taylor Knopf
The free water sampling tests are available 8 a.m.to 5 p.m. at the New Hanover County Government Center, Suite 140, 230 Government Center Drive, or at the New Hanover County Fire Department, Station 11 in Wrightsboro at 3515 North Kerr Ave.
The kits include instructions. Residents must bring the well water sample within 24 hours of collecting the sample to New Hanover County Public Health laboratory, 2023 S. 17th St., Wilmington. If the well sample tests positive for fecal coliform bacteria, the Environmental Health division will follow up with treatment options.
The Craven County Health Department based in New Bern also is offering free well water test kits to homeowners, who can visit the health department to receive the kit and paperwork. Samples can be dropped off at the health department from 8 a.m. to 4 p.m. Monday through Thursday.
Results will be provided to the homeowner and if the well is contaminated, then the homeowner will be informed of a course of action. For more information, contact the Environmental Health Department at 252-636-4936.
For Carteret County residents, the county Environmental Health Department is offering free bacteriological samples for private drinking water wells flooded during the hurricane. After flooding around the well has receded and power has been restored, disinfect and chlorinate the well prior to requesting sampling. Instructions are on the county website. Sampling can be requested by contacting 252-728-8499. Environmental Health staff will visit to collect a sample.
In the North Carolina counties hit hardest by Hurricane Florence, people who already get help buying food will be given more, and those not on a state or federal food program can receive assistance going forward, federal and state officials said Thursday.
The announcement follows by a few days a visit to the state by U.S. Department of Agriculture (USDA) Secretary Sonny Perdue, who arrived Monday to hear more about Florence’s devastation from Gov. Roy Cooper, Commissioner of Agriculture Steve Troxler and Secretary of Environmental Quality Michael Regan. Torrential rains from the storm brought destruction and weeks of flooding to some counties that hadn’t completely recovered from Hurricane Matthew’s 2016 destructive visit.
Help is on the way for people who qualify for the federal Disaster Supplemental Nutrition Assistance Program (D-SNAP). Families will have a one-time deposit placed on a special debit card, with the amount based on the size of the household.
“We want to do everything we can to help families recover from Hurricane Florence,” state NC Department of Health and Human Services Secretary Dr. Mandy Cohen said in a statement. “This program will help people who have suffered losses buy food for their families as they begin the long process of rebuilding their lives.”
As an example, DHHS said, a family of one would receive $192, a family of four would get $640 and bigger families would get more.
The state Department of Health and Human Services listed the counties as Bladen, Beaufort, Brunswick, Carteret, Columbus, Craven, Cumberland, Duplin, Harnett, Hoke, Hyde, Johnston, Jones, Lee, Lenoir, Moore, New Hanover, Onslow, Pamlico, Pender, Pitt, Richmond, Robeson, Sampson, Scotland, Wayne and Wilson.
Sponsored
“Our department is committed to providing the assistance needed to our neighbors, as they pull themselves to recovery,” Perdue said in a statement. “The D-SNAP program USDA is announcing today is an important step forward in bringing back normalcy to those impacted.”
Tailored by county
Some groups of counties are covered by special provisions. The help will come in several different forms.
For people in Bladen, Brunswick, Carteret, Columbus, Craven, Duplin, Harnett, Hoke, Hyde, Jones, Lee, Moore, New Hanover, Onslow, Pamlico, Pender, Richmond, Robeson, Sampson and Scotland counties:
++ Everyone who already gets help from the federal Food and Nutrition Service, commonly known as “food stamps,” will automatically have 60 percent of their monthly deposit replaced on their electronic benefit transfer (EBT) card.
++ A number of households in the affected counties will get additional spending power on their EBT cards if they don’t already get the maximum amount based on the size of their households.
++ People or households who experienced loss of food that cost more than 60 percent of their benefit for September can apply for a larger replacement from their county Department of Social Services.
In Beaufort, Cumberland, Johnston, Lenoir, Pitt, Wayne and Wilson counties:
People on the FNS program who have experienced food loss can ask to have a portion of their benefits for September replaced. Households that experienced loss of food and receive less than the maximum benefit can apply for additional amounts from their county Department of Social Services. They’ll need to complete an affidavit available at county DSS offices.
Who’s eligible for D-SNAP?
To be eligible for the Disaster-Supplemental Nutrition Assistance Program an applicant must:
Live in a disaster-declared county.
Apply in person between Friday, Sept. 28, and Oct. 6.
Be prepared to wait at state-designated D-SNAP locations (below).
Be a victim of damage from Florence in areas such as property damage, lost income or food supplies.
If available, show proof of identity and residency.
Have levels of income and worth below certain guidelines.
Source: North Carolina DHHS
County
Physical Address
Times of Operation
Beaufort
Beaufort County Department of Social Services, 632 West Fifth St., Washington, NC 27889
Mon. – Fri.: 8 a.m.-6 p.m.
Sat.: 9 a.m.-5 p.m.
Chocowinity Fire Department, 512 NC 33 Chocowinity, NC 27817
Fri., Sept. 28: 8 a.m.-6 p.m.
Sat., Sept. 29: 9 a.m.-5 p.m.
Aurora Community Center, Main St., Aurora NC 27806
Fri., Sept. 28: 8 a.m.-6 p.m.
Sat., Sept. 29: 9 a.m.-5 p.m.
White Plains Church, 718 Pine St., Belhaven, NC 27810
Fri., Sept. 28: 8 a.m.-6 p.m.
Sat., Sept. 29: 9 a.m.-5 p.m.
Bladen
Bladen County DSS, 208 E McKay St., Elizabethtown, NC 28337
8:30 a.m.-6:30 p.m., Mon. – Sat.
NC Cooperative Extension, 450 Smith Circle, Elizabethtown, NC 28337
8:30 a.m.-6:30 p.m, Mon. – Sat.
Bladenboro Fire Department, 519 West Seaboard St., Bladenboro, NC 28320